
More Related Content
What's hot
What's hot (20)
Similar to Arthrogryposis
Similar to Arthrogryposis (20)
More from Dr.Avinash Rao Gundavarapu
More from Dr.Avinash Rao Gundavarapu (20)
Recently uploaded
Recently uploaded (20)
Arthrogryposis
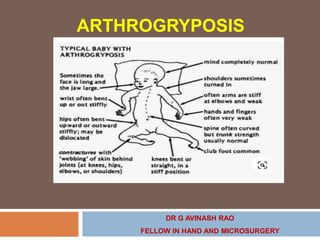
- 1. ARTHROGRYPOSIS DR G AVINASH RAO FELLOW IN HAND AND MICROSURGERY
- 4. INTRODUCTION 1st depicted in 1841 by A.W. Otto, he called - congenital myodystrophy. Subsequently termed “multiple congenital contractures” by Schantzin 1897, Arthrogryposis” by Rosenkranz. Greek, literature - meaning "curving of joints" (arthron "joint"; grȳpōsis "hooking / bent"). Arthrogryposis Multiplex Congenita term coined by WG Stern in 1923 Scheldonin 1932 described clinical features of congenital multiple contractures in a child and used for the first time the name “amyoplasia congenita” Other terms were amyoplasia congenita and congenital arthromyodysplasia
- 5. Pathological Anatomy Arthrogryposis affects the entire musculoskeletal system. Children with arthrogryposis have absent or hypotrophic muscles but may retain the associated tendons and overlying fascia. As the child grows, these noncontractile tissues can tether the joints, which may lead to joint contractures. Because the bones do not have the normal load of muscle activity or weight bearing, they may be severely osteopenic.
- 6. Cortices in these children tend to be quite thick, but the bones are of small diameter and the medullary canal is nearly absent. The motor and mixed nerves are also small in caliber compared with those in other children of the same size. With thin bones and a hypoplastic musculature, the subcutaneous fat encompasses - a larger than expected percentage of the bulk of the arms.
- 7. DEFINITION The term arthrogryposisis used to denote non progressive conditions characterized by multiple joint contractures found at birth & It involves contractures of at least two joints in two different body regions. Incidence: Varies Considerably (from country to country) Any child with congenital joint contractures in two or more limbs can be classified as having arthrogryposis multiplex congenita (AMC); the term does not specify any certain cause for the contractures.
- 8. Arthrogryposis can result from environmental or genetic causes but is most often idiopathic with wide range of levels of severity and anatomic involvement. Arthrogryposis can also result from myriad disorders that compromise the central or peripheral nervous system or the musculature; currently, over 300 types have been identified. Muscles are either absent or hypoplastic, often replaced by fibrofatty tissue. Tendons and overlying fascia are often preserved even when no muscle is present, leading to tethering at the joints.
- 9. Children with amyoplasia have a characteristic appearance with high cheeks and button noses and “stork bite” hemangiomas over the occiput and the bridge of the nose. Children tend to have average to above average intelligence. Terminal limb deficits are more common in amyoplasia patients than in the general population. The family history is usually positive in DA and in other inheritable neuromuscular conditions, but it is otherwise
- 10. Etiology It usually occurs due to absence of active fetal movements (akinesia), normally appearing in the eighth week of fetal life Fetal akinesia lasting over 3 weeks may be sufficient to result in absence of normal stretching of muscles and tendons acting on the affected joints, and cause reduced compliance of the joint capsule and periarticular ligaments Consequently fetal akinesia leads to fibrosis and contractures of the affected joints determined by the passive position of the limb. The direct etiological factor causing akinesia in humans remains unknown.
- 11. Hall’s Classification of AMC 1) Primarily Limb Involvement 2) Limb involvement+ other body areas. 3) Limb + CNS involvement
- 12. Pathogenesis – Intrinsic Factors Maternal Considerations 1. Multiple Sclerosis 2. Diabetes Mellitus 3. Myasthenia Gravis 4. Maternal Infection 5. Maternal Hyperthermia 6. Drug Exposure 7. Myotonic Dystorphy Intrauterine Vascular Compromise 1. Severe bleeding 2. Failed termination 3. Monozygotic twins 4. Amniotic Bands Neurologic Deficit 1. Disorders of Cerebrum 2. Anterior Horn Cell deficiency 3. Abnormalities of nerve function or structure (central and peripheral) Genes resulting in abnormal development of myocytes - congenital muscular dystrophy Connective Tissue/Skeletal Deficit 1. Primary disorder of joint/connective tissue 2. Diastrophic dysplasia. 3. Collagen disorders - Larsen's syndrome, multiple pterygium syndrome, congenital arachnodactyly, and Beals syndrome
- 13. Pathogenesis – Extrinsic Factors 1) Intrauterine mechanical obstruction 2) Fetal crowding: multiple births 3) Oligohydramnios 4) Uterine myomas 5) Amniotic bands 6) Trauma
- 14. Genetics of Arthrogryposis Arthrogryposis is a group of clinical symptoms that can be observed in many different genetic syndromes : 1) Sporadic 2) Single-gene mutations (e.g. autosomal dominant, autosomal recessive and X-linked recessive inheritance patterns). 3) Chromosomal disorders (e.g. trisomy 18) such as deletion, translocation, or duplication, and mitochondrial disorders.
- 15. Approach to diagnosis Family history Pregnancy history Delivery history Physical exam Multidisciplinary approach
- 16. Upper limb Shoulder Adducted and internally rotated. Deltoid muscle function is deficient. Elbow Extension contracture of the elbows with deficient brachialis and biceps brachii function, resulting in absent or significantly deficient elbow flexion. Flexion contracture of the elbow is less commonly observed. The elbow joint is cylindrical in appearance and devoid of any skin creases . Forearm in neutral to slight pronation
- 17. Wrist Characteristic palmar flexion contracture with ulnar deviation and pronation of the hand. Patients with myogenic arthrogryposis / DA may present with extension contracture of the wrist. Hand Flexion contractures of interphalangeal joints (most common). Metacarpophalangeal joints relative extension contractures. Thumb is usually adducted. Finger contractures are usually stiff and most patients have significant deficiency of active finger movements In syndromic arthrogryposis - “clenched fist” with “thumb in palm” deformities may be observed.
- 18. Lower limb Hip 1. Mostly flexion, abduction, and external rotation contractures of varying degrees of severity. 2. Unilateral or bilateral hip dislocation is observed in approximately 1/3 of patients. Knee – 1. The most common deformity is flexion contracture of varying severity, Flexion contracture is usually associated with weak quadriceps and a “dimple” over the patella. 2. An extension contracture is less commonly observed and may be accompanied by knee dislocation.
- 19. Ankle joint And Foot These deformities are observed in nearly all arthrogryposis patients. Severe talipes equinovarus (most common). Less frequently vertical talus observed. These deformities are characterized by usually extreme severity, difficulties in treatment and high tendency to relapse. Spine Abnormal curvatures in approximately 28% to 67% of patients Simple long thoracolumbar curves without concomitant vertebral malformations The curves often rapidly progress.
- 20. Extra skeletal manifestations Facial skeleton – Hypoplasia of the mandible (micrognathia). Contracture and limited function of temporo-mandibular joints. Extraskeletal clinical signs and symptoms Normal intelligence Hemangioma on the forehead. Abdominal wall abnormalities(inguinal hernia or gastroschisis) Varying abnormalities of the reproductive.
- 21. DISTAL ARTHROGRYPOSIS Inheritance is autosomal dominant Contractures limited mainly to the distal portions of the limbs, i.e. to wrists, hands, ankles, and joints of the foot. Contractures of other joints are low-degree or absent. According to Bamshad 10 types of distal arthrogryposis had been described The most common DAs are types 1, 2A, and 2B (DA1, DA2A, and DA2B.
- 22. Bamshad M, Van Heest AE, Pleasure D: Arthrogryposis: a review and update. J Bone Joint Surg Am 91(Suppl 4):40–46, 2009.
- 23. Other Arthrogryposis Pterygium syndromes These are a separate class of genetically mediated congenital contractures, characterized by the presence of pterygia: these are skin webs located in the area of a joint and causing limitation of its range of motion. Skin webs may also be found in lateral portions of the neck, and be accompanied by cleft palate or lip, syndactyly or atypical fingerprints. Many variations have been described with varying inheritance patterns of clinical features including autosomal dominant or recessive, e.g. lethal Bartsocas-Papas syndrome
- 24. Escobar's syndrome (multiple pterygium syndrome) Neck webs are evident at birth but are not always severe. Clinically the Escobar syndrome is characterized by facial dysmorphism, neck (bucco- sternal) webs, and hand contractures. With age, the neck webs may increase in size; the neck mobility is limited due to concomitant congenital vertebral malformations. The lumbar lordosis increases with age as well; in adolescence, lumbar lordosis and popliteal and cubital webs increase in size. The inheritance pattern is autosomal recessive, sometimes autosomal dominant; the syndrome may be associated with mental retardation. The lethal multiple pterygium syndrome is autosomal recessive; features include severe contractures, hypertelorism, cervical pterygia, narrow chest, and hypoplastic lungs.
- 26. Larsen syndrome A genetically mediated, autosomal dominant syndrome with an incidence of 1/100,000 live births, caused by a mutation of the gene encoding filamin B (FLNB), a component of the actin complex in the cell protein cytoskeleton. The clinical features of Larsen syndrome may include multiple contractures, most commonly in the form of talipes equinovarus. The dominant features are hypermobility and congenital dislocations of multiple joints: hips, knees, and elbows. Cervical spine instability and kyphosis may be present, leading to potentially life-threatening cervical cord injuries. Other features include: laryngomalacia and/or subglottic stenosis, low body stature, central facial hypoplasia, and accessory metacarpal and metatarsal bones. Mental development is usually normal.
- 27. .
- 28. Bruck syndrome Extremely rare, autosomal recessive form of arthrogryposis, with combined clinical features of osteogenesis imperfecta and congenital contractures; this disease was historically described by Alfred Bruck in 1897
- 32. Investigations Routine radiographs are unnecessary for patients with arthrogryposis. Some experts advocate lateral finger radiographs to evaluate phalangeal condyle hypoplasia in cases of camptodactyly. Neither computed tomography nor magnetic resonance imaging is necessary for the diagnosis or treatment of AMC. Electrodiagnostic studies are rarely necessary other than in evaluating specific neurogenic contracture syndromes. Muscle biopsy rarely yields useful information unless a specific, unusual diagnosis is being pursued.
- 33. Treatment The principal treatment goal in arthrogryposis is optimization of quality of life: this includes communication capabilities, unassisted activities of daily living, social participation capacity, independent ambulation, and consequently independent living. In order to achieve these goals, management must be initiated as early as possible, and optimally in the neonate and infant.
- 34. The goal of any treatment plan for a child with arthrogryposis is to maximize functional independence for that child. For the lower extremities, the goals are ambulation and sitting. For the upper extremity, the primary goals are to have “one hand to eat and one to wipe.” They can be by the same hand. The child must be able to acquire the food and Grip it firmly enough to bring it to the mouth, and release it. Beyond that, the wrist and the elbow combined must have enough extension to reach the plate or the table and sufficient flexion to allow the hand to reach the mouth. Forearm and shoulder rotation need to allow the hand to face the plate and then the mouth.
- 35. Perineal care can be performed through the legs or around the back. Children who wipe their buttocks through the legs require wrist flexion, elbow extension, and shoulder internal rotation. Children who wipe their buttocks around the back require forearm supination, elbow extension, and shoulder extension.
- 36. This comprehensive approach is based on a triad of treatment tools: Firstly, rehabilitation including physiotherapy, manipulation of contractures, and later social and occupational rehabilitation. Secondly, individually tailored orthotic management, whether for maintenance or correction of joint mobility, and for prevention of recurrent deformities. Thirdly, a broad spectrum of surgical techniques for correction of musculoskeletal deformities, typically found in congenital contractures
- 37. Rehablitation and Physiotherapy The parents of a child with arthrogryposis often place the greatest importance on independent ambulation and concentrate their attention on this ability in the treatment program . It is therefore extremely important that the treatment plan and its objectives – both immediate and long-term – be communicated to both the patient and the parents. At birth - Gentle stretching and ROM exercises Passive stretching exercise followed by serial splinting with custom made thermoplastic splints
- 38. Existing joint motion to be preserved and placed in most functional position Stiff joints placed for functional advantage 2 major goals Plantigrade standing and walking Restoring function of upper limb to carry out daily living activities
- 39. Shoulder Typically present with adduction and internal rotation contracture. Capsular releases – not helpful. Best – Derotation Osteotomy of humerus. Contraindication - Absence of pectoralis function. Children who lack pectoralis function but retain triceps function will use an obligatory crossover grasp pattern that requires internal rotation. Medial / DeltoPectoral / anterolateral / Posterior approach. Desired position of between neutral and 15 degrees of internal rotation - Sufficient internal rotation should be preserved to allow for midline function, such as perineal care
- 42. For the child with a severe elbow extension contracture (<30 0 of elbow flexion) distinguishing between an internal rotation contracture at the elbow and a pronation contracture at the forearm can be difficult. For these children, we will perform an elbow release first, followed by a humeral rotational osteotomy. Bilateral procedures in these children rarely performed because the margin of error is so small for losing midline function. Complications - Overrotation or underrotation is the most common complication. Typically, younger children will correct for overrotation but will not correct for underrotation
- 43. Elbow Range of motion exercises ,Early splinting & Serial casting. Stiff flexed – surgery not indicated Elbow Extension Contractures : One side to be treated at a time Posterior capsulotomy and triceps tendon lengthening Transfer of triceps, pectoralis, or latissimus dorsi to maintain Elbow stability in extension. Steindler flexorplasty Improves active flexion if passive flexion ≥ 90 °
- 44. Elbow – Extension Contacture Release Elbow Flexion < 30 - Caretakers and health care professionals are discouraged from performing passive range of motion of these elbows because inadvertent collateral ligament damage or physeal injuries. Elbow Flexion > 30 - Impressive gains in elbow range of motion can be made with Passive ROM. Indications for surgical release - less than 30 degrees of elbow flexion by 12 to 18 months of age and failure to achieve sufficient elbow flexion for self-feeding at any age. Contraindicated - contralateral side elbow flexion contracture that prohibits perineal care and Absent Triceps function ( flexion contracture).
- 45. Posterior approach (Dominant Hand First)– Ant.Transposition of Ulnar Nerve Distally based V-Y advancement – IF INADEQUATE - Turndown flap / Autograft /allograft. Additional Release of Medial head of Triceps all the way upto Spiral groove subperiostially – Helps. Flexion if inadequate – Perform Ant.Closed Wedge Humeral Osteotomy proximal to Olecronon fossa. Release till flexion is B/W – 90 – 120 degree. Hour-Glass Splint Maintains the Flexion. Avoid Forceful Elbow Flexion – might cause Transphyseal Fractures.
- 46. Complications – Triceps Insufficiency and Elbow Stiffness.
- 47. In a child with passive motion who would benefit from active elbow flexion, there are several options for achieving active flexion. Transfer of the entire triceps to the biceps has proven to be a poor option. Transferring only the long head of the triceps – proponents of this technique have yet to demonstrate a substantial improvement. Other options for restoring active elbow flexion are a Steindler flexorplasty, a unipolar or bipolar pectoralis major transfer, a bipolar latissimus dorsi transfer, and a free muscle transfer. When present, the latissimus dorsi is the best choice for restoring active elbow flexion
- 48. Bipolar Latissimus Dorsi Transfer Contraindicated – Poor / Absent Triceps function due to previous lengthening and Passive ROM of elbow < 90 degree. Expected outcome – power of 3+ and above can be achieved. It depends on the quality of harvested LD. As long as the latissimus dorsi is in good condition, the bipolar latissimus muscle transfer is a fairly reliable technique for achieving active elbow flexion. Another viable option is a free gracilis with a spinal accessory nerve transfer.
- 49. Wrist Wrist Deformities: Volar flexion and ulnar deviation Splinting shortly after birth Surgical indication - For fixed wrist contractures interfering with function Release of: Volar wrist capsule. Flexor Carpi Ulnaris tendon transfer to Extensor Carpi Radialis Brevis. Osteotomy of distal radius. Intracarpal extension osteotomy. Post-op splinting ….. to improve dorsiflexion. Arthrodesis - Near skeletal maturity in slight palmar flexion.
- 50. Radial Osteotomy With And Without Ulna Osteotomy Forearm in case of Arthrogryposis – most ofen Neutral. It is Performed in cases of forearm pronation contracture. Differentiate between shoulder internal rotation contracture and forearm pronation contracture – to avoid mismanagement. It is difficult to differentiate both in case of elbow contracture in extension . So, before doing humerus or forearm osteotomy – perform an elbow release. A radial osteotomy is usually sufficient for rotational correction below 45 degrees. Beyond that, an ulnar osteotomy can be added for corrections up to 90 degrees. Alternatively, a onebone forearm is more predictable and easier to accomplish.
- 51. Contraindicated - A child who requires pronation for perineal care should not undergo a neutralization osteotomy of the forearm. A one-bone forearm is the most predictable operation for correcting forearm rotational deformities. Union in children is rapid and robust, and there is no risk of loss of correction over time. Correction of a pronation deformity can be a life-changing event if it allows the child to self-feed for the first time. If it takes away or prohibits the acquisition of independence in the bathroom, Loss of forearm pronation can have lifelong consequences.
- 52. Carpal wedge osteotomy The carpal wedge osteotomy is a common upper limb procedure for children with arthrogryposis. However, the indications are few and the contraindications are many. Decisions about altering a child’s wrist position require a thorough assessment of the child’s overall functional goals and limitations Most patients with DA tend to have wrist extension contractures, whereas patients with amyoplasia have flexion contractures. Surgical interventions in the wrist and hand have not been demonstrated to have better outcomes at a younger age, surgery can be delayed until the child’s functional needs and capabilities are better defined
- 53. Extension contractures at the wrist are well tolerated if the following criteria are met: (1) Finger extension is sufficient to acquire and release objects, (2) Forearm supination and elbow flexion are sufficient to get food to the mouth. (3) Forearm supination, shoulder extension, and elbow extension are sufficient to be able to wipe the perineum from behind.
- 54. If the child has good finger extension and has sufficient pronation and elbow flexion to reach the mouth without the need of wrist flexion, and can perform perineal care around the back, the most reliable procedure to provide wrist extension is a carpal wedge osteotomy with ECU to ECRB transfer. The osteotomy cut should correct both wrist ulnar deviation and flexion. The best candidates for this - reciprocal deformity of wrist flexion and MP extension. In cases where one hand is to be used for wiping and the other for eating, the eating hand can be considered for a carpal wedge osteotomy.
- 55. Contraindications - to correcting a child’s wrist flexion contracture 1. Poor finger extension in maximal preoperative wrist extension, 2. Obligatory wrist flexion for hand-to-mouth movement, 3. Obligatory wrist flexion for perineal care, 4. Use of the back of the wrist for scooting along the ground for ambulation or for balance and support during standing or sitting. 5. Complications – Undercorrection, Loss of finger extension and increased finger stiffness, Nonunion (rare).
- 58. Thumb
- 60. Thumb Reorientation and Metacarpophalangeal Chondrodesis The classic clasped thumb in arthrogryposis consists of extension at the first carpometacarpal (CMC) joint and flexion at the MP joint. This is more commonly seen in distal arthrogryposis. CMC joint generally follows the position of the wrist. Children with wrist flexion contractures, as are more commonly seen with amyoplasia, typically have CMC joint flexion contractures with the MP joint in extension. Surgical options should seek to place the thumb in a position where it can best provide pinch and / or grasp, regardless of appearance. Thumb reorientation osteotomy is used to correct CMC flexion. Thumb MP chondrodesis is used to correct MP flexion.
- 62. Patients with no digital motion usually lack any active motion in the upper extremity. If FPL function is preserved despite no other function - The thumb orientation prevents useful prehension, and these patient are good candidate for a thumb reorientation osteotomy. The goal of the osteotomy is to place the thumb into a position where it can best take advantage of the child’s existing finger and thumb motion to provide pinch and / or grasp. Both type 1 and type 2 thumbs benefit from a first web space contracture release at the same time as a chondrodesis or reorientation osteotomy.
- 63. MP chondrodesis alone will not address a CMC flexion contracture. A combination of MP chondrodesis and reorientation osteotomy may be required. Using a reciprocating saw, make an incomplete transverse osteotomy just distal to the physis. Referencing the thumbnail, make a second cut to create a dorsal closing wedge at the desired angle Complete both cuts. Reduce the osteotomy by extending, abducting, and pronating the thumb
- 65. The stiletto flap is the workhorse flap for the thumb in arthrogryposis, allowing both expansion of the first web and resurfacing of the volar MP joint. It is rare in these children to require only first web space expansion - so a four-flap Z-plasty or an Abdel Ghani flap is less often used. For children with fixed thumb-in-palm deformities who can flex their fingers over the thumb, the standard operation is the Thumb MP chondrodesis with first web space expansion. The functional and aesthetic gains are typically dramatic, and most patients will ask for the same operation on the contralateral side once they realize the results.
- 66. For children whose fingers do not reach the thumb and a thumb that does not reach the palm, pinch is not possible without reorientation of the thumb. The fingers must actively flex sufficiently to reach the thumb in its planned position in order to achieve postoperative pinch. Contraindications – Fixed extension contracture at the CMC joint that would preclude opposition after the MP chondrodesis. Children with stiff fingers that would not reach the thumb even after reorientation or MP fusion are not candidates for thumb surgery.
- 68. Camptodactyly Release Camptodactyly is more common in DA and can be a defining characteristic of specific syndromes such as Beals syndrome (contractural arachnodactyly). Camptodactyly can interfere with capturing objects in the hand, with some children developing a compensatory pinch-and-grasp pattern against the dorsum of the contracted fingers
- 69. Radiographs are not useful for camptodactyly in young children. In older children, the condyles at the PIP joint will often appear hypotrophic Children with passively correctable camptodactyly are more likely to have well formed condyles than children with fixed flexion contractures. In general, the more severe the condylar hypoplasia, the less correctable the deformity.
- 70. Standard treatment for camptodactyly is releasing the pterygium by Z-plasty along with FDS tenotomy (if the FDP is functional and the FDS is tight ). If the camptodactyly is passively correctable and there is good FDS excursion, the FDS can be transferred to the lateral band to augment the extensor mechanism. Results of camptodactyly release are unpredictable, despite some favorable results in the literature. It is rare that a patient will be worse off, unless one is attempting extensor mechanism augmentation.
- 71. Contraindications - A relative contraindication for FDS tenotomy is lack of the flexor digitorum profundus (FDP) and intrinsic function. Complications - Stiffness is the most common complication after any camptodactyly release. Digital nerve injury and vascular injury are possible and are most often traction injuries caused by straightening a bent finger.
- 72. Summary Arthrogryposis remains a challenging disease for the patient, the parents, and the treating practitioner. Fortunately, the initial joint contractures tend to improve over time with stretching and splinting. Each child follows his or her own path, however with some returning to full function and other less fortunate children never developing any muscle tone. There is little margin for error in these children, and parents should be aware that any surgical intervention may risk compromising existing function. Surgery should be pursued only if the potential benefits in function outweigh the potential losses.
- 73. Operating on one arm at a time provides a mechanism for the surgeon, patient, and family to judiciously assess the outcome. Although the options are often limited and the results of surgery are not always predictable, helping these children transition from dependence to independence is tremendously rewarding. Sterling Bunnell’s famous words, “To someone who has nothing, a little is a lot” particularly apply to these children.