Temporomandibular joint disorders
•
5 likes•221 views

TMJ disorders from oral medicine view

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Temporomandibular joint disorders
Similar to Temporomandibular joint disorders (20)
More from Eman Alsheikh
Recently uploaded
Recently uploaded (20)
Temporomandibular joint disorders
- 2. INTRODUCTION • Temporomandibular joint (TMJ) is a unique joint in which translatory as well as rotational movements are possible & where both the ends of bone articulate, in the same plane, with that of other bone. • It is also called as ginglymodiarthrodial type of joint, meaning that it has a relatively sliding type of movement between bony surfaces, in addition to hinge movement, common to diarthrodial joint.
- 3. COMPONENTS OF TEMPOROMANDIBULAR JOINT a) Glenoid Fossa & Articular Eminence/ Protuberance b) Mandibular Condyle c) Articular Capsule and Articular Disk d) Synovial Fluid e) Discal Ligaments f) Posterior Attachment or Retrodiscal Tissue or Bilaminar Zone g) Ligaments Associated with TMJ h) Muscles of Mastication i) Arterial Supply, Venous Drainage & Sensory Innervation of TMJ
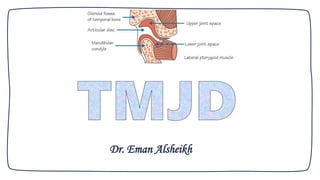
- 4. • The structure of the TMJ• (A) Upper joint space; (B) lower joint space; (C) interarticular disc; (D) condylar head; (E) lateral pterygoid muscle superior head; (F) lateral pterygoid muscle inferior head (G) mandibular fossa; (H) articular eminence; (I) external auditory canal
- 5. Skeletal components of TMJ (condylar head & the glenoid fossa).
- 7. The biconcave articular disk. Courtesy: Dr Arturo Mann
- 8. Schematic diagram showing the location of the temporalis & masseter muscle Schematic diagram showing the medial pterygoid muscle Schematic diagram showing the medial pterygoid muscle
- 12. TMJD • Temporomandibular disorders (TMD) are characterized by craniofacial pain involving the joint, masticatory muscles, or muscle innervations of the head & neck. TMD is a major cause of nondental pain in the orofacial region. • TMD affects 10% to 15% of adults, but only 5% seek treatment. • The incidence of TMD peaks from 20 to 40 years of age; it is twice as common in women than in men & carries a significant financial burden from loss of work.
- 13. • Symptoms can range from mild discomfort to debilitating pain, including limitations of jaw function. • The most common syndromes are: myofascial pain disorder, disk derangement disorders, osteoarthritis, & autoimmune disorders.
- 14. Etiology • The etiology of TMD is multifactorial & includes: 1. Biologic, 2. Environmental, 3. Social, 4. Emotional, 5. Cognitive triggers. • Factors consistently associated with TMD include other pain conditions (e.g., chronic headaches), fibromyalgia, autoimmune disorders, sleep apnea, and psychiatric illness.
- 15. A study showed a twofold increase in TMD in persons with depression & an increase in myofascial pain in persons with anxiety. Smoking is associated with an increased risk of TMD in females younger than 30 years.
- 16. Classification
- 17. In 2013, the International Research Diagnostic Criteria for TMD Consortium Network published an updated classification structure for TMD. TMD is categorized as: 1. Intra-articular (within the joint) 2. Extra-articular (involving the surrounding musculature)
- 18. 1. Articular disorders (intra-articular) 1. Congenital/developmental disorders 2. Degenerative joint disorders 3. Disk derangement disorders 4. Infection 5. Neoplasia 6. TM hypermobility 7. TM hypomobility 8. Trauma a) Condylar hyperplasia b) First and second branchial arch disorders c) Idiopathic condylar resorption a) Inflammatory: capsulitis, synovitis, polyarthritides (rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Reiter syndrome, gout) b) Noninflammatory: osteoarthritis a) Displacement with reduction b) Displacement without reduction (closed lock) c) Perforation a) Dislocation b) Joint laxity c) Subluxationa) Ankylosis: true ankylosis (bony or fibrous) or pseudoankylosis b) Postradiation fibrosis c) Trismus a) Contusion b) Fracture c) Intracapsular hemorrhage
- 19. 2. Masticatory muscle disorders (extra-articular) 1. Local myalgia 2. Myofascial pain disorder 3. Myofibrotic contracture 4. Myositis 5. Myospasm 6. Neoplasia
- 20. Examination A. Clinical Examination B. Radiology C. Arthroscopy
- 21. A. Clinical Examination: The dental examination should be systematic & include the TMJ & the masticatory muscles. 1) Joint examination 2) Muscle examination
- 22. Joint examination Movement: Face the patient and ask him/her to open slowly to maximum. Normal range (interincisal) is 35–40 mm. If opening is thought to be reduced, ask whether the limiting factor is pain or an obstruction. Note the path of opening and any lateral deviation. Pain on palpation: Palpate in front of the ear & within the external auditory meatus.
- 23. Joint examination Auscultation: This needs a stethoscope to be done properly. However, clicks may well be audible without a stethoscope. A click implies a disc displacement that reduces into a normal position on opening. Crepitus (cracking/grating noise) implies degenerative change or, sometimes, acute inflammation.
- 24. Muscle examination Muscle tenderness suggests some abnormal function (clenching, bruxism). I. Masseter & temporalis muscles are assessed by direct palpation. II. The lateral pterygoid is indirectly examined by noting the response (in terms of any preauricular pain) to attempted opening against the restriction of the examiner’s hand below the chin. III. The medial pterygoid cannot be examined.
- 25. Radiology Most clinical problems related to the TMJ are caused by muscular parafunction (e.g. bruxism) or internal disc derangements. Neither is likely to be associated with any relevant bony abnormalities. So, radiography is not normally indicated unless there is any suggestion of bony abnormality, such as might be the case in rheumatoid arthritis or osteoarthrosis.
- 26. Radiology A clinical diagnosis of suspected internal derangement might lead to a requirement for imaging of the disc. 1) Panoramic X-ray 2) magnetic resonance imaging (MRI)
- 27. Arthroscopy Arthroscopy allows visual examination of the upper joint space and an opportunity for minor surgical treatment. A small arthroscope can be used to facilitate lavage & division of joint adhesions. The lower joint space is difficult to access without risk of damage to the articular disc. Arthroscopy is undertaken under local anesthesia; however, if lengthy arthroscopic surgery is to be undertaken, then a conscious sedation technique would be appropriate or even general anesthesia.
- 28. Common disorders of the joint
- 29. 1) Pain/dysfunction • The most common TMJ disorder is pain or dysfunction. Clinical features Symptoms are a combination of: • Headache • Limitation/deviation of jaw opening • Joint sounds • Pain on palpation of the TMJ • Pain on palpation of the associated muscles. Joint sounds alone, or with headache, are not diagnostic of TMJ pain/dysfunction.
- 30. Radiology There is no abnormality visible. Management • Reassurance & explanation to patients. • Jaw rest & soft diet. • Analgesics/anti-inflammatory drugs. • Occlusal splints to interfere with parafunction may offer some help. • Physiotherapy. • Muscle relaxants.
- 31. 2) Internal derangement The articular disc normally sits above the anterior aspect of the condylar head, with the disc posterior attachment lying within 10° of the vertical. A disc may be anterior to this ‘normal’ position in asymptomatic individuals, suggesting that an anterior disc position is a normal variant.
- 32. 2) Internal derangement Thus, an internal derangement is best thought of as an abnormality in position that interferes with function & that may be associated with other symptoms. An anterior disc ‘displacement’ is the most common internal derangement, but anteromedial, medial, & anterolateral displacements are all seen.
- 34. 3) Disc displacement with reduction • Reduction means that a displaced disc ‘reduces’ into a normal position on opening but reverts to an abnormal position on closing (reciprocal click). • Clinical features: 1. Clicking on opening. 2. Clicking on closing. 3. Transient jaw deviation during opening/closing
- 35. Radiology • No abnormalities are apparent on plain radiographs. • MR imaging shows the displaced disc in a closed/rest position
- 36. (A) A displaced disc with reduction showing the movement diagrammatically (B) On MRI in closed & open positions closed open (B) (A)
- 37. Management 1. Consider no treatment other than reassurance & explanation. 2. Occlusal splints to interfere with parafunction may offer some help. 3. Physiotherapy: It should be emphasized that treatment should only be considered where the abnormality is affecting the patient’s quality of life; a clicking joint may be considered as normal
- 38. 4) Disc displacement without reduction • If there is no reduction, a displaced disc remains in a displaced position regardless of the stage of opening. • This interferes with movement & may cause pain. • Clinical features: 1. Reduction in opening. 2. In unilateral cases, lasting deviation on opening. 3. No click. 4. Pain may be present in front of the ear
- 39. Radiology • Plain films usually show nothing. • In long-standing cases, there may be signs of osteoarthrosis. • MR imaging shows an abnormal disc position in all movements • In long-standing cases, perforation of the disc may be seen & joint space adhesions inferred
- 40. (A) A displaced disc without reduction showing the movement diagrammatically & (B) on MR in closed and open positions
- 41. Management • Explanation of the condition and reassurance. • Muscle relaxants and physiotherapy. • Manipulation under anesthetic. • TMJ surgery.
- 42. Other conditions affecting the joint
- 43. 1) Osteoarthrosis 2) Rheumatoid arthritis 3) Juvenile “chronic” rheumatoid arthritis 4) Trauma 5) Effusion 6) Dislocation 7) Ankylosis Other conditions affecting the joint
- 44. Osteoarthrosis Osteoarthrosis is a non-inflammatory disorder of joints in which there is joint deterioration with bony proliferation. The deterioration leads to loss of articular cartilage & bone erosions. The proliferation manifests as new bone formation at the joint periphery and subchondrally.
- 45. It has an unknown etiology, but previous trauma, parafunction & internal derangements are all suggested as etiological factors. C/F: 1) Pain localized to the TMJ region. 2) Limitation of opening, worse with prolonged function. 3) Crepitus. 4) Tender on palpation of TMJ.
- 46. Radiology • Plain films show: 1. Erosions of the articular surfaces of the condyle &, less commonly seen, of the mandibular fossa. 2. Sclerosis of the bone & marginal bony proliferation (‘lipping’ or osteophytes) are & narrowing of the radiographic joint space. 3. Bony proliferations may break away & be seen as loose bodies in the joint space.
- 47. Radiograph of osteoarthrosis showing marginal bony proliferation (‘lipping’)
- 48. Management • Explanation & reassurance. • Anti-inflammatory drugs. • Physiotherapy. • Restore deficiencies in the posterior occlusion to reduce loading on TMJs. • Intra-articular steroid injections (advanced disease). • Surgery (advanced disease; final option) to smooth irregular condylar head where there are osteophytes or irregularities.
- 49. Rheumatoid arthritis Rheumatoid arthritis is a disorder associated with synovial membrane inflammation in several joints.
- 50. C/F: • Pain over TMJs. • Tenderness over TMJs. • Swelling over TMJs. • Stiffness & limitation of opening. • Crepitus. • Developing anterior open bite & retrusion of chin in advanced disease. • Joints of hands, wrists, knees & feet commonly involved.
- 51. Radiology Radiology demonstrates reduction in bone density in the TMJ. There is marked erosion of the condylar head & articular fossa & narrowing of the joint space. In long-standing disease, there is: • Destruction of entire condyle • Anterior open bite • Secondary osteoarthrosis • Ankylosis.
- 52. Management: • Analgesics/anti-inflammatory drugs. • Steroids. • Physiotherapy
- 53. Juvenile chronic (rheumatoid) arthritis Juvenile chronic rheumatoid arthritis differs from rheumatoid arthritis in the age of onset (mean age 5 years), the severe systemic involvement & the absence (in some cases) of rheumatoid factor. While it shares clinical & radiological features with rheumatoid arthritis, the age of onset means that there is often a severe effect on mandibular growth, leading to a ‘bird face’ appearance owing to the mandibular retrusion, often accompanied by an anterior open bite.
- 54. The disease often has periods of remission/quiescence, during which time the erosions of the joint may ‘smooth over’ with formation of a new cortex. Ankylosis may occur.
- 55. Effusion Effusion is influx of fluid into the joint, usually either bleeding following trauma or inflammatory exudate. C/F: • Pain over joint. • Swelling over joint. • Limitation of movement. • Sensation of a blocked ear. • Difficulty in occluding posterior teeth.
- 56. Radiology There is a widened joint space. Management • Anti-inflammatory drugs. • Rarely, surgical drainage may be needed.
- 57. Dislocation In dislocation of the TMJ, the condyle is abnormally positioned outside the mandibular fossa but within the joint capsule. Dislocation may occur during trauma or be caused by failure of muscular coordination.
- 58. C/F: • Inability to close the jaw. • Pain. • Muscle spasm.
- 59. Radiology Radiography confirms a clinical diagnosis. • The condyle may translate beyond the articular eminence normally, without a dislocation, so clinical information is essential. • The condyle will be anterior and superior to the ‘summit’ of the articular eminence.
- 60. Management • Manual manipulation to reduce the dislocation. • Intravenous sedation with midazolam provides muscle relaxation & greatly facilitates this maneuver. • The patient should avoid wide mouth opening for some days & use the hand to prevent this when yawning.
- 61. Manual manipulation to reduce a dislocated jaw.
- 62. Ankylosis Fusion across a TMJ may occur as a result of trauma, mastoid infection or juvenile chronic arthritis. Surgical treatment is by joint replacement with a prosthetic joint unless the patient’s facial development is not yet complete, when a costochondral (rib) graft is used in an attempt to provide a bony replacement that may grow.
- 63. MCQs • Temporomandibular joint is a unique of (a) Ginglymodiarthrodial type (b) Diarthrodial type (c) Synarthrodial (d) Amphiarthrodial
- 64. • Diagnostic criteria for MyoFacial pain dysfunction syndrome are except: (a) Unilateral pain (b) Muscle tenderness (c) Clicking (d) Radiographic evidence
- 65. Short Question • Classify TMJ disorders. • Enumerate various traumatic disorders of TMJ. • Write in detail about clinical features, radiological features and management of Disc displacement without reduction.
- 66. Case -1- An 11-year-old patient, following trauma to the jaw as an infant, developed a worsening facial asymmetry and now has extreme limitation of opening. He has no other joint problems in the body. 1. What diagnosis is suggested? 2. What would be the management?
- 67. Case -2- A 35-year-old woman with a long history of clicking and occasional pain from her right TMJ presents with an acute event, consisting of limited opening, deviation of the jaw towards the affected side on attempted opening and pain localized to the joint region. These symptoms were present upon waking up in the morning and have been unchanged since. She mentions that the click that has always been there is no longer present. 1. What diagnosis is suggested? 2. What would be the management?
- 68. Hello! THANKS