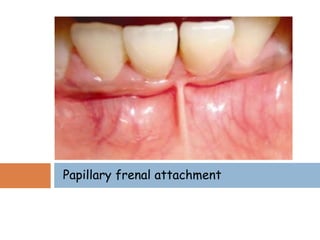
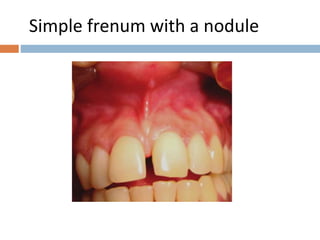
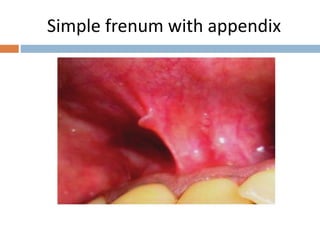
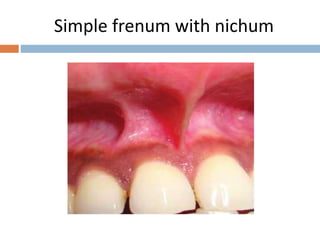
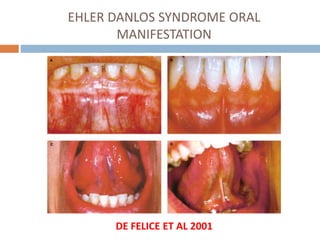
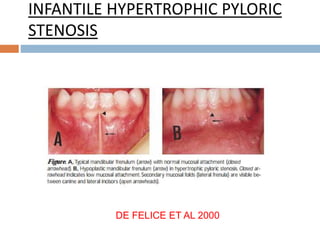
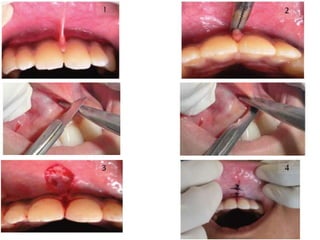
This document discusses the frenum attachment in the oral cavity, its development and variations. It describes different types of frenum attachments and associated syndromes like Ehlers-Danlos syndrome. Complications of an abnormal frenum like gingival recession and difficulty brushing are mentioned. Treatment techniques for abnormal frenum like frenectomy and frenotomy using conventional, Z-plasty, and laser methods are summarized. Post-operative instructions are provided.