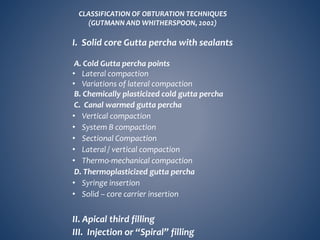
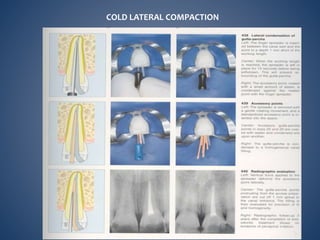
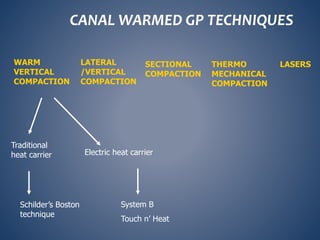
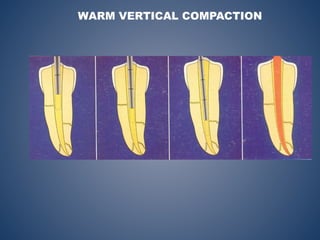
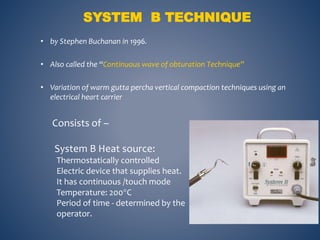
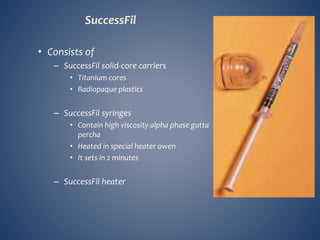
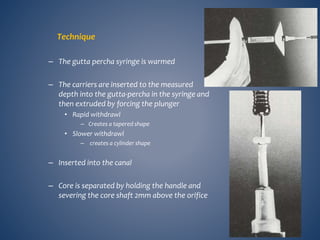
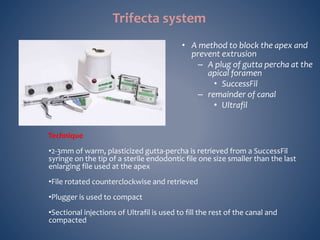
This document discusses obturation techniques in endodontics. It begins with defining obturation and its objectives, which are to eliminate leakage and seal any irritants remaining in the root canal. Next, it classifies root canal filling materials and lists the ideal requirements of core materials and sealers. The document then describes various obturation techniques including cold lateral compaction, chemically plasticized gutta percha, and various warm gutta percha techniques like vertical compaction and thermo-mechanical compaction. It provides details on techniques like System B and Touch n' Heat and concludes by stating that controlling heat and filling voids are important aspects of obturation.