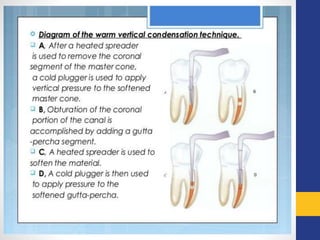
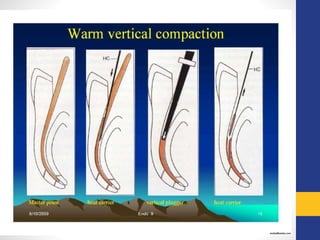
Obturation is the process of filling and sealing the root canal system. It involves placing a root canal sealer and core filling material into the cleaned and shaped root canal. The goals of obturation are to achieve a fluid-tight seal of the root canal to prevent reinfection. Common materials used for obturation include paper points, gutta percha, and sealers. Techniques for obturation include cold lateral condensation, warm condensation (vertical or lateral), and thermoplasticized gutta percha.