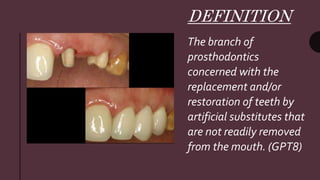
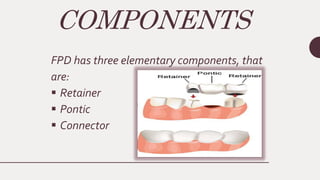
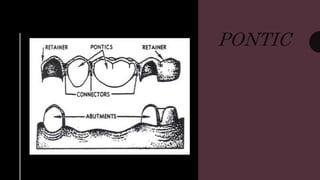
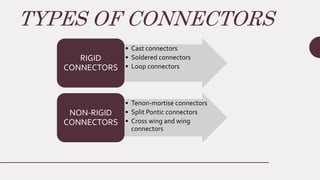
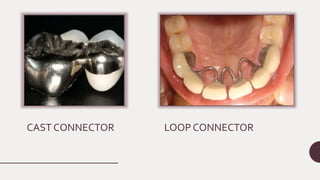
This document discusses the key components of a fixed partial denture (FPD), including retainers, pontics, and connectors. It defines each component and describes their classification and ideal requirements. For retainers, it covers types based on tooth coverage and retention mechanism, as well as criteria for selection. Pontic types include those with and without mucosal contact. Connectors are categorized as rigid or non-rigid, with examples like cast, soldered, and loop connectors. The document provides indications, advantages, and disadvantages of different retainer, pontic, and connector designs.









![[Crown & Bridges] [terminology & classification]](https://cdn.slidesharecdn.com/ss_thumbnails/lec01-02terminologyclassification-151105130852-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






