Download to read offline


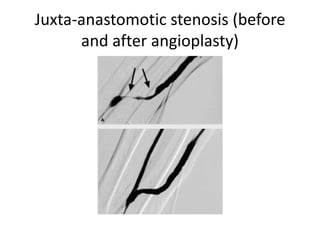





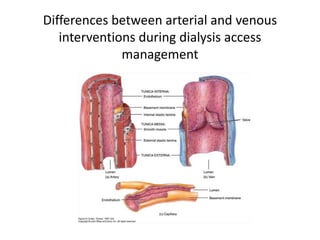
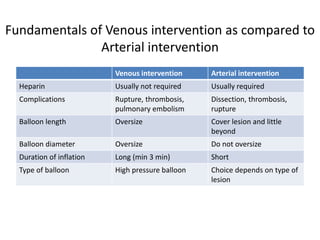


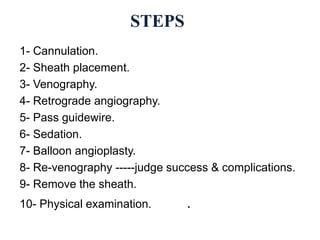
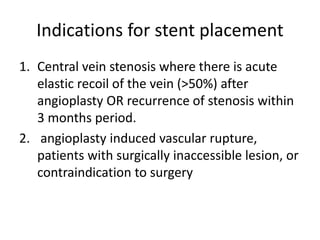
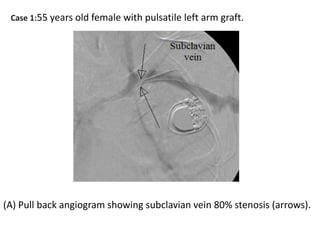
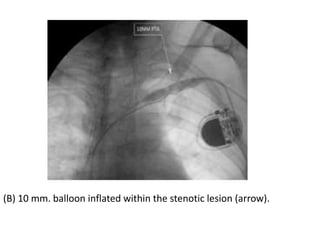
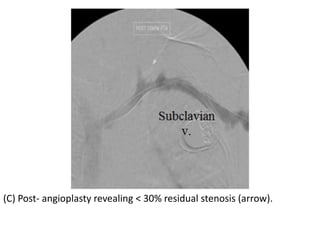
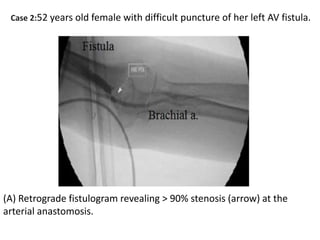
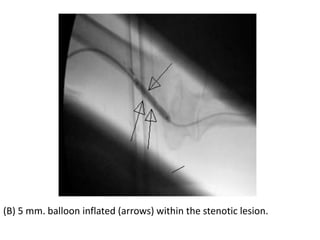
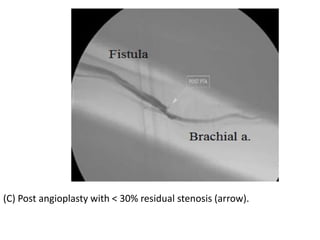
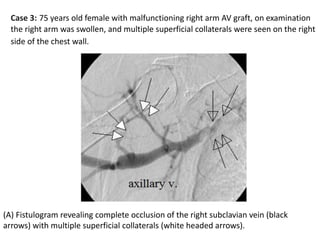
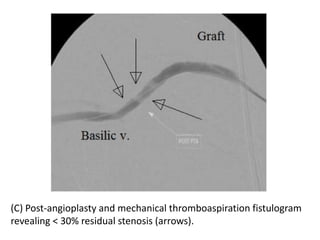
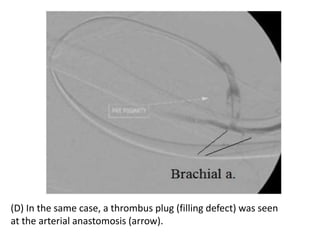
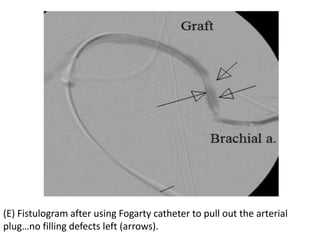


The document discusses strategies for salvaging failing vascular access in hemodialysis patients through techniques like balloon angioplasty and stent placement. It outlines the complications associated with vascular access and guidelines for monitoring access. Examples are provided of endovascular interventions performed to treat stenoses in arteriovenous fistulas and grafts.























































































