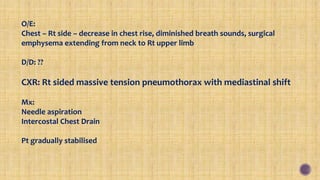
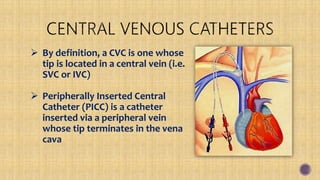
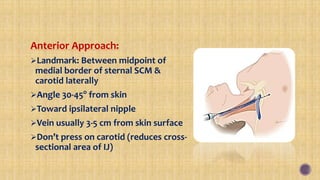
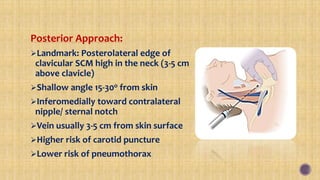
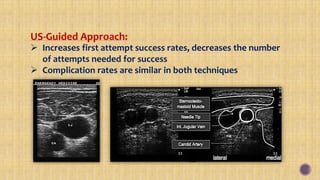
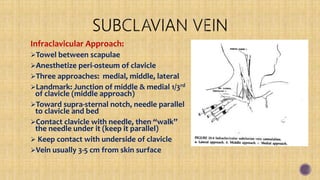
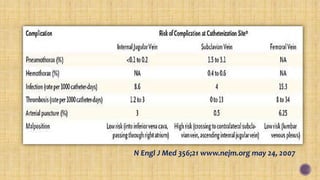
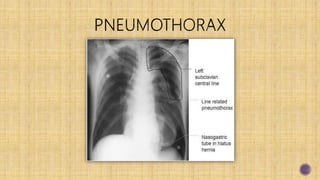
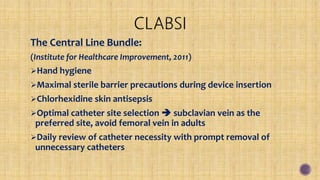
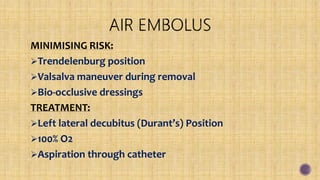
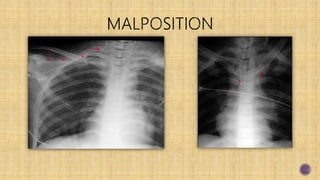
The document details a critical case of a 72-year-old male patient in the ICU with multiple medical conditions who undergoes various interventions including intubation due to respiratory failure and a suspected tension pneumothorax. It provides extensive information about central venous access techniques, indications, contraindications, and complications associated with various catheter placements. Additionally, it discusses guidelines to minimize risks during central line procedures, emphasizing the importance of trained supervision and patient assessment post-procedure.