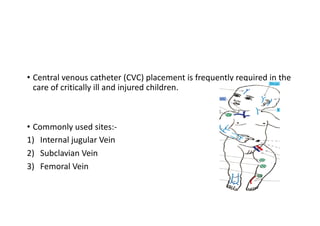
Central venous catheters (CVCs) are commonly used in critically ill children for medication administration, monitoring, and other purposes. The document discusses CVC insertion techniques and sites, including the internal jugular, subclavian, and femoral veins. Proper insertion involves strict sterility, ultrasound guidance when possible, local anesthesia, and confirming proper placement to avoid complications like bleeding, infection, and accidental arterial puncture.