Downloaded 37 times


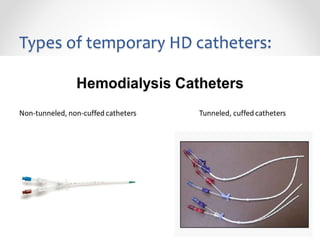

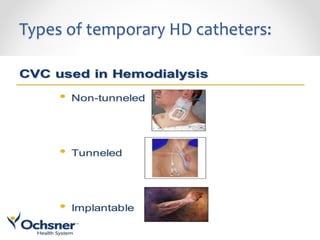
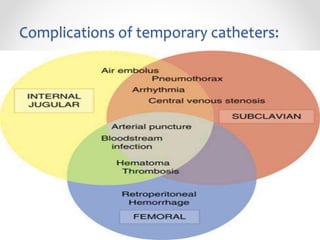
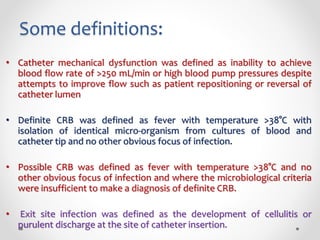
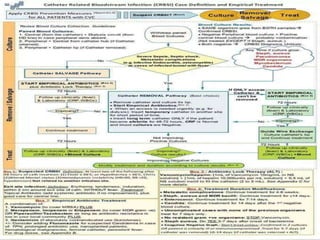


This document provides guidance on the use of temporary hemodialysis catheters. It discusses indications for temporary catheters such as acute kidney injury or as a bridge to renal transplantation. Types of temporary catheters and precautions before insertion are outlined. The document also reviews care after insertion, common complications, and how to manage catheter-related bloodstream infections. The overall message is that arteriovenous fistula is preferred for end-stage renal disease patients requiring long-term hemodialysis, but temporary catheters have a role when fistula is not ready or in cases of acute kidney injury.




































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















