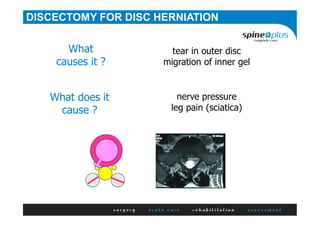
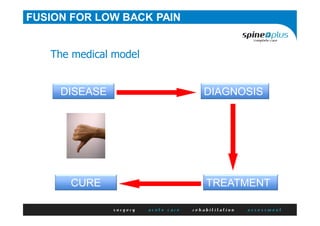
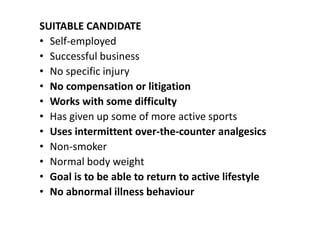
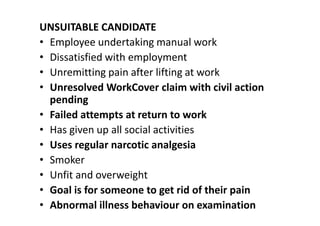
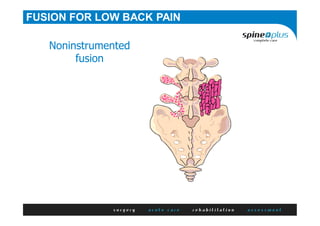
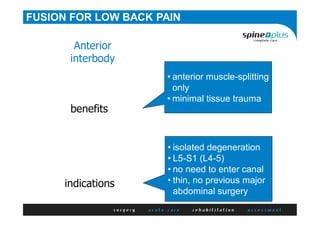
This document discusses different types of back surgery for low back pain, including discectomy and spinal fusion. It provides details on discectomy for disc herniation, including causes, symptoms, prerequisites for surgery, expected outcomes, and the surgical procedure. For spinal fusion, it notes the procedure is generally only good for low back pain if there is a specific diagnosis, clearly defined pain source, suitable patient candidate without psychosocial factors, and an appropriate surgical technique is used to address the underlying pathology. Results are not as good for fusion compared to discectomy or for non-specific low back pain. The document also discusses factors that make a patient suitable or unsuitable for fusion surgery.