
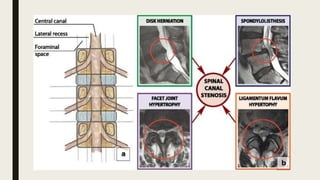
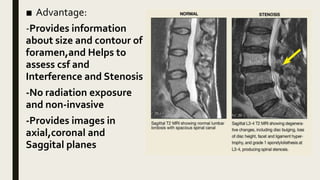



1. Spinal stenosis is the narrowing of spaces in the spinal canal which can compress the spinal cord and nerve roots. It most commonly occurs in the lumbar region and is caused by degenerative changes in the spine over time including disc bulging and thickening of ligaments. 2. Symptoms include neurogenic claudication which is pain, numbness, or weakness in the legs that worsens with standing or walking and improves with bending forward or sitting. MRI is the preferred imaging test to evaluate the severity and location of narrowing. 3. Treatment begins with non-surgical options like medications, physical therapy, and epidural steroid injections but may require surgical decompression if conservative measures fail. Common surgical









































































