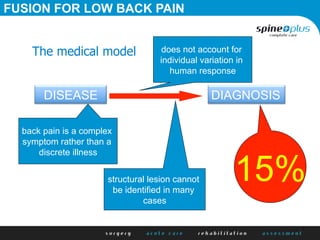
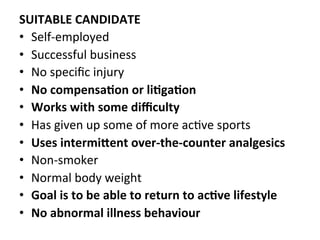
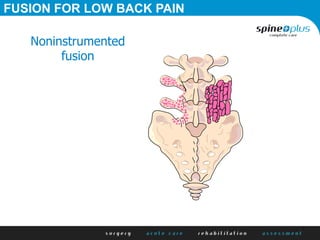
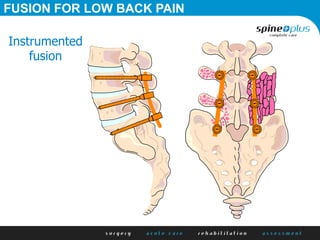
The document discusses various surgical options for low back pain, emphasizing the differences between discectomy and fusion procedures. It highlights the effectiveness of discectomy in most cases while pointing out that fusion outcomes are generally less favorable. The suitability of candidates for fusion surgery is also assessed based on their individual circumstances and psychosocial factors.