Downloaded 19 times









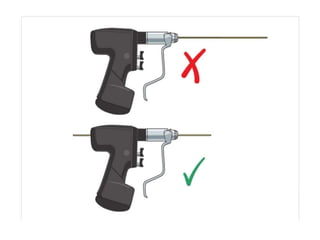

















































K wires are commonly used in orthopedic surgery to fixate small bone fractures and dislocations. They were introduced in 1909 and are made of stainless steel or nickel titanium alloy. K wires are inserted using fluoroscopic guidance to stabilize bone fragments while allowing early range of motion. Proper technique and wire placement is important to avoid complications like loss of fixation, infection, or stiffness.























































































