Downloaded 311 times

![CLASSIFICATION OF SUPRAGLOTTIC
AIRWAY
BASED ON EVOLUTION
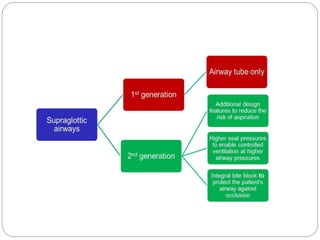
First-generation devices: Simple airway tubes
1. The laryngeal mask airway [classic LMA (cLMA)],
2. flexible LMA (fLMA),
3. unique LMA (ULMA) and
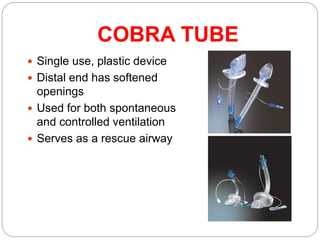
4. The Cobra Perilaryngeal Airway (CobraPLA)
Second-generation devices: With addition of
Drainage tube
1. Proseal LMA (PLMA),
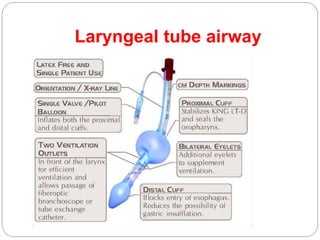
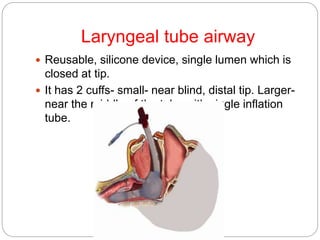
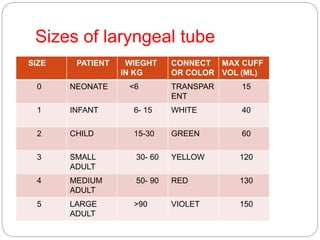
2. i-gel, Laryngeal tube,
3. LMA Supreme,
4. Streamlined Liner of the Pharyngeal Airway](https://image.slidesharecdn.com/supraglotticairwaychildren-150602065721-lva1-app6891/85/Supra-glottic-airway-children-5-320.jpg)




This document discusses supraglottic airway devices in children. It provides a history of the first supraglottic device, the LMA, introduced in 1988. It defines supraglottic devices and classifies them based on sealing mechanisms and generation. The document discusses indications, contraindications, advantages, and limitations of supraglottic devices in children. It provides details on insertion and placement of LMAs and describes different types of LMAs including the classic LMA, ProSeal LMA, flexible LMA, i-gel, and air-Q intubating laryngeal airway.























































































