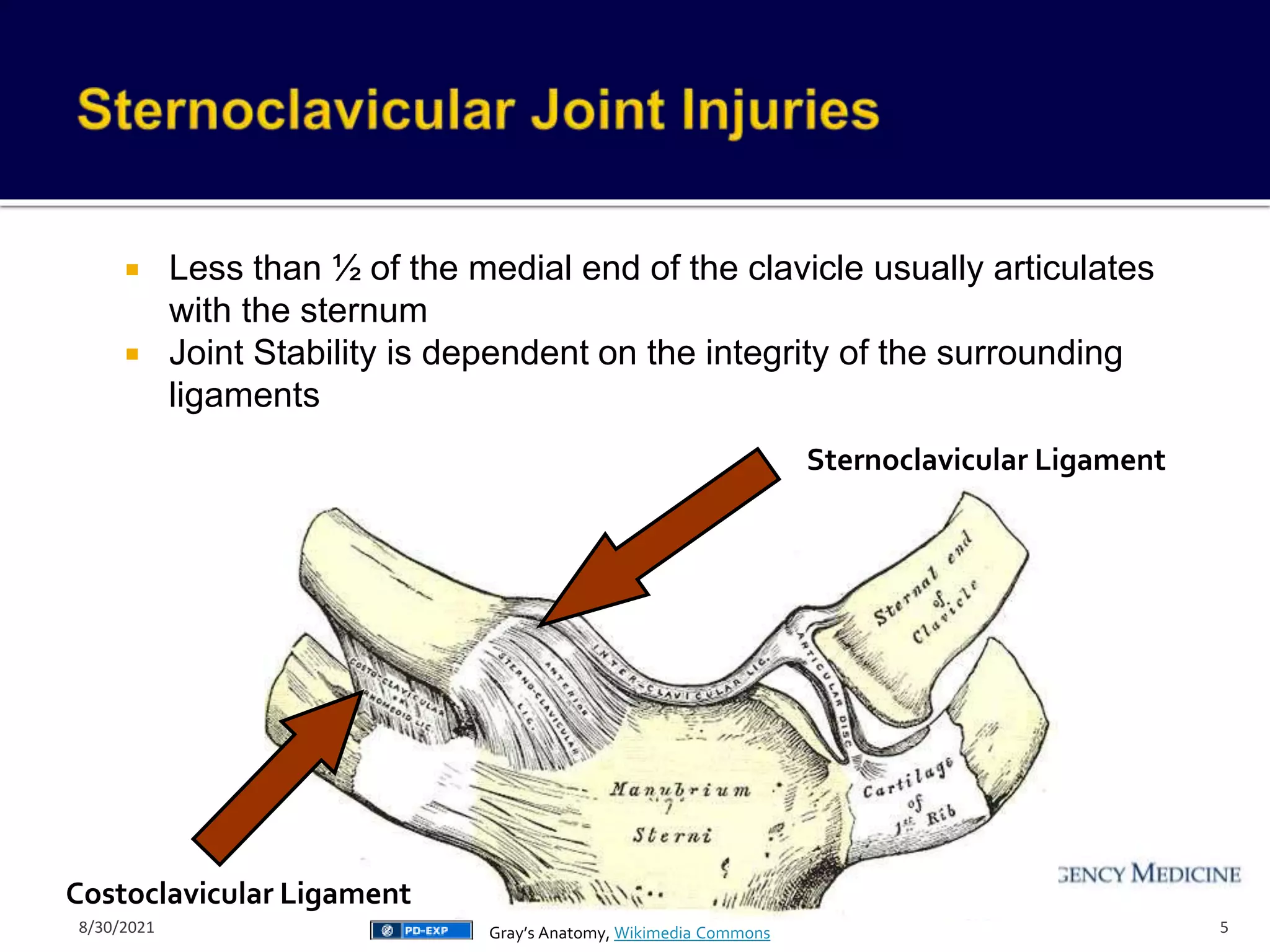
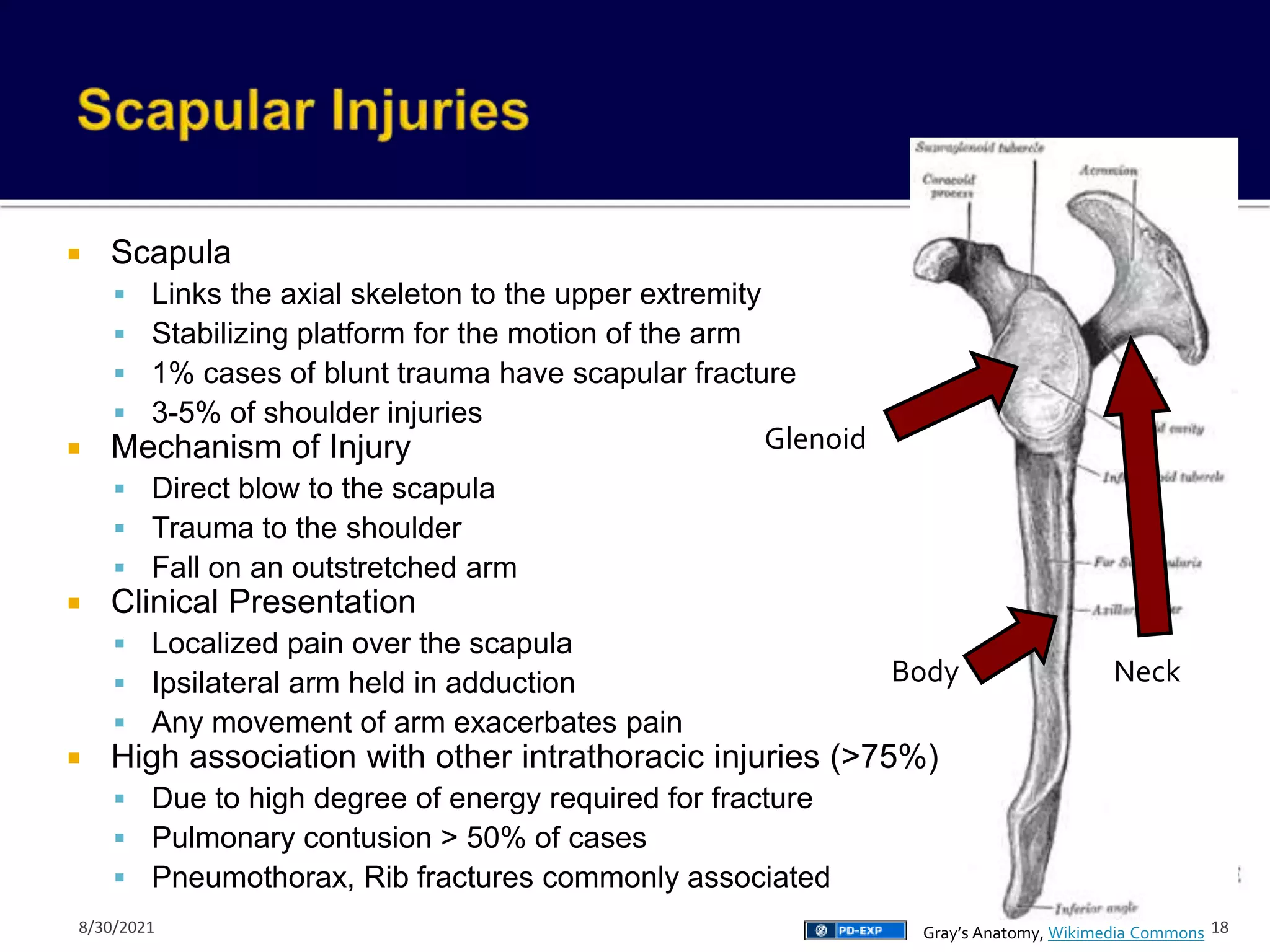
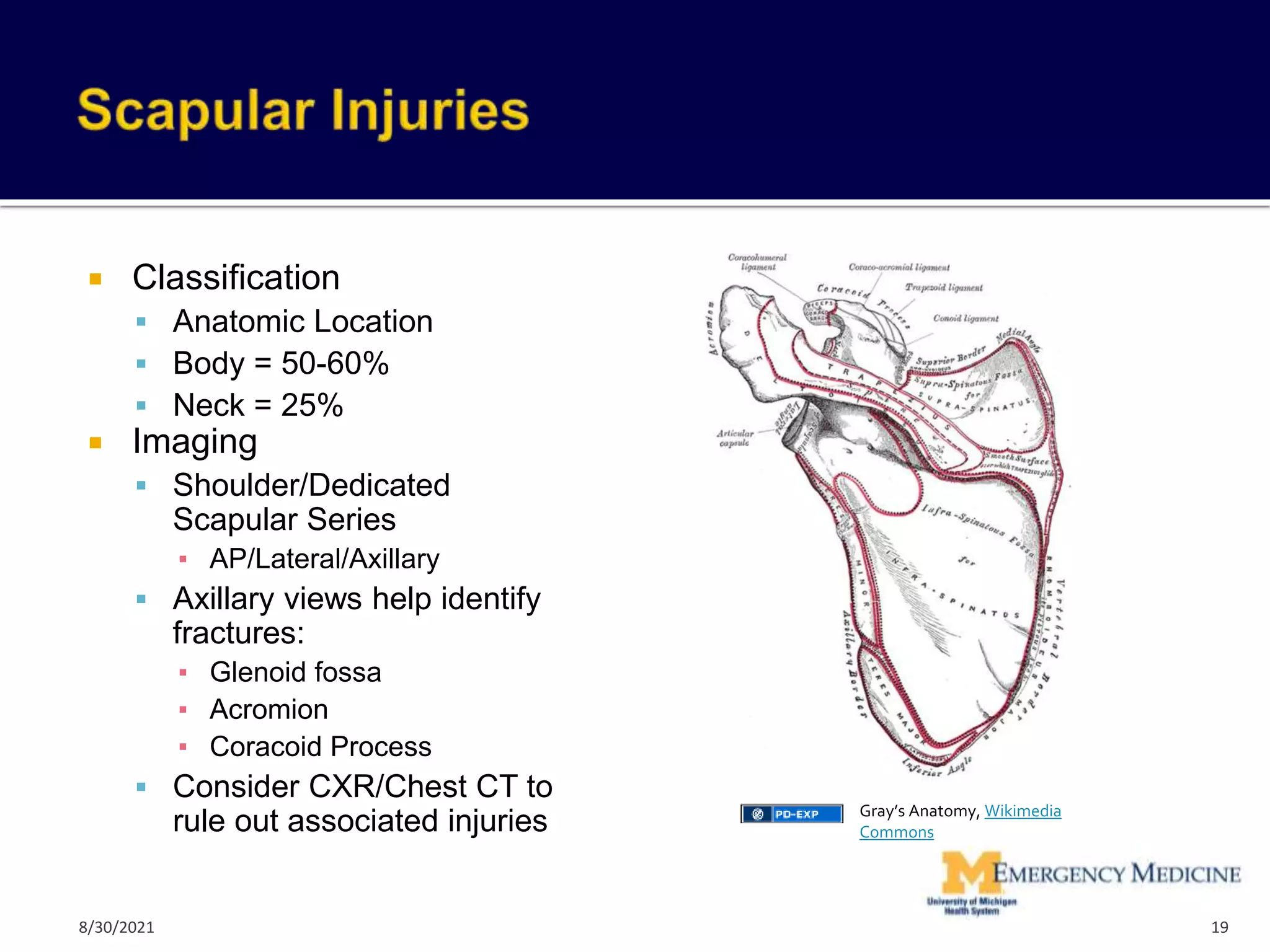
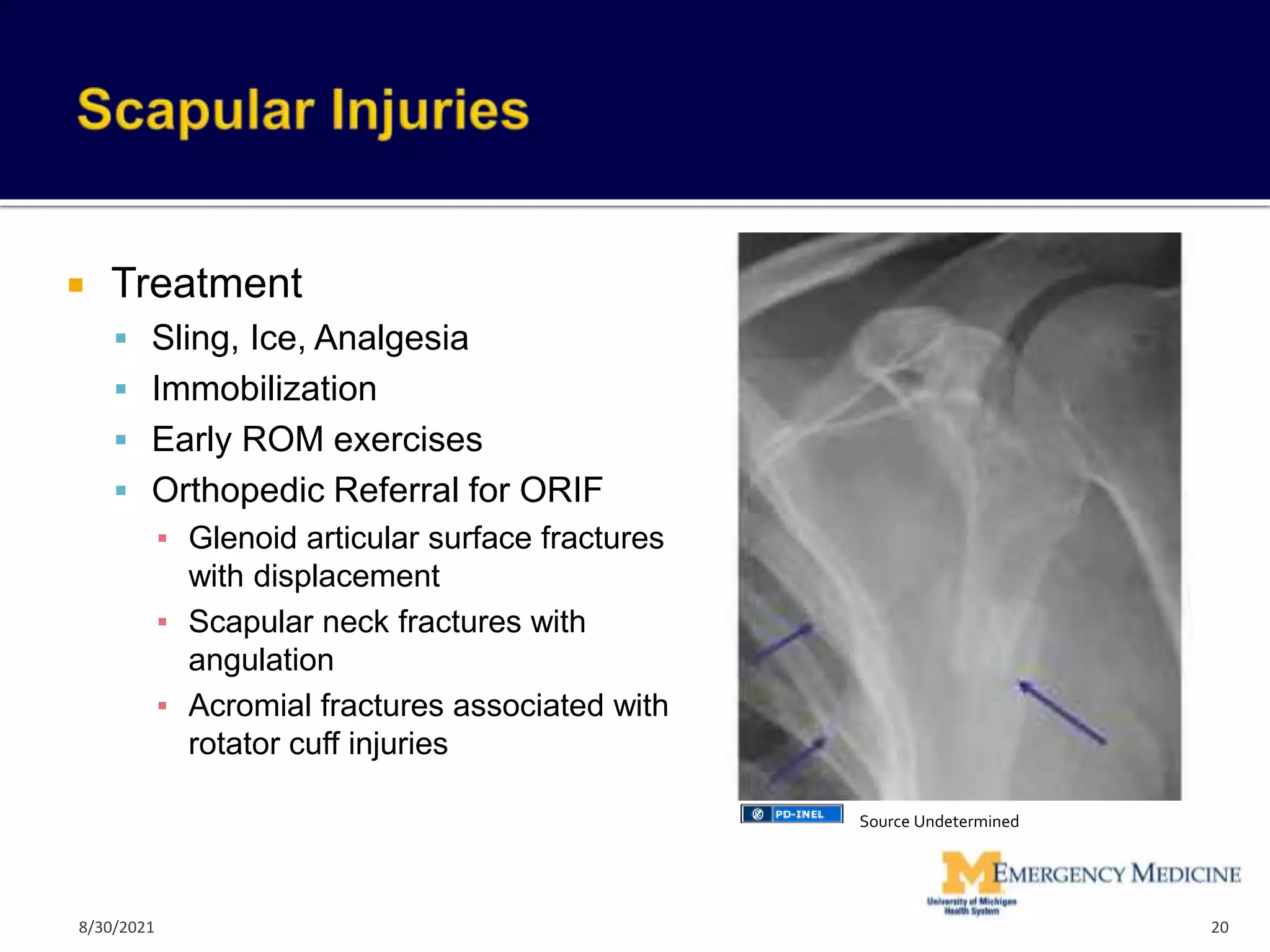
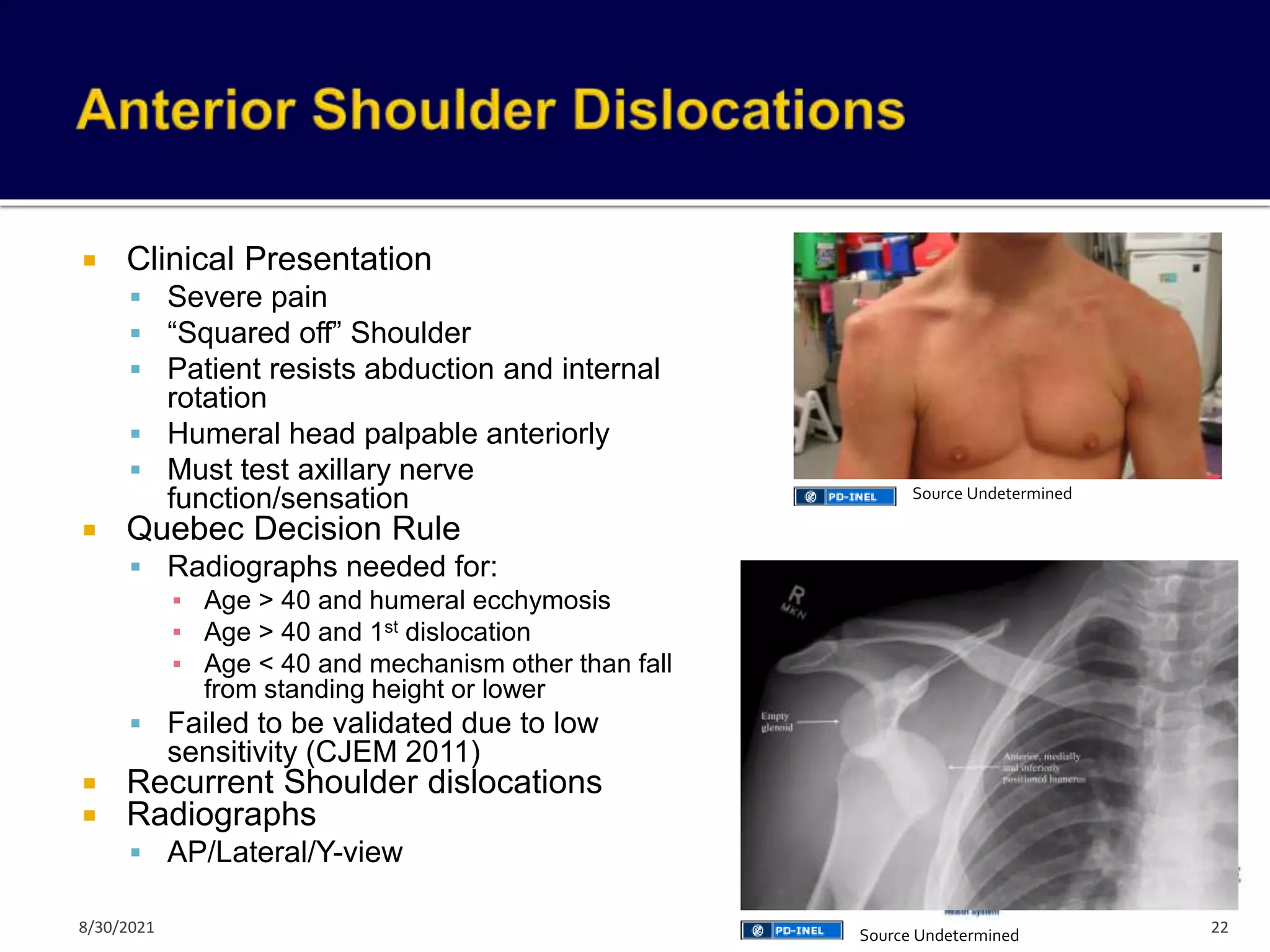
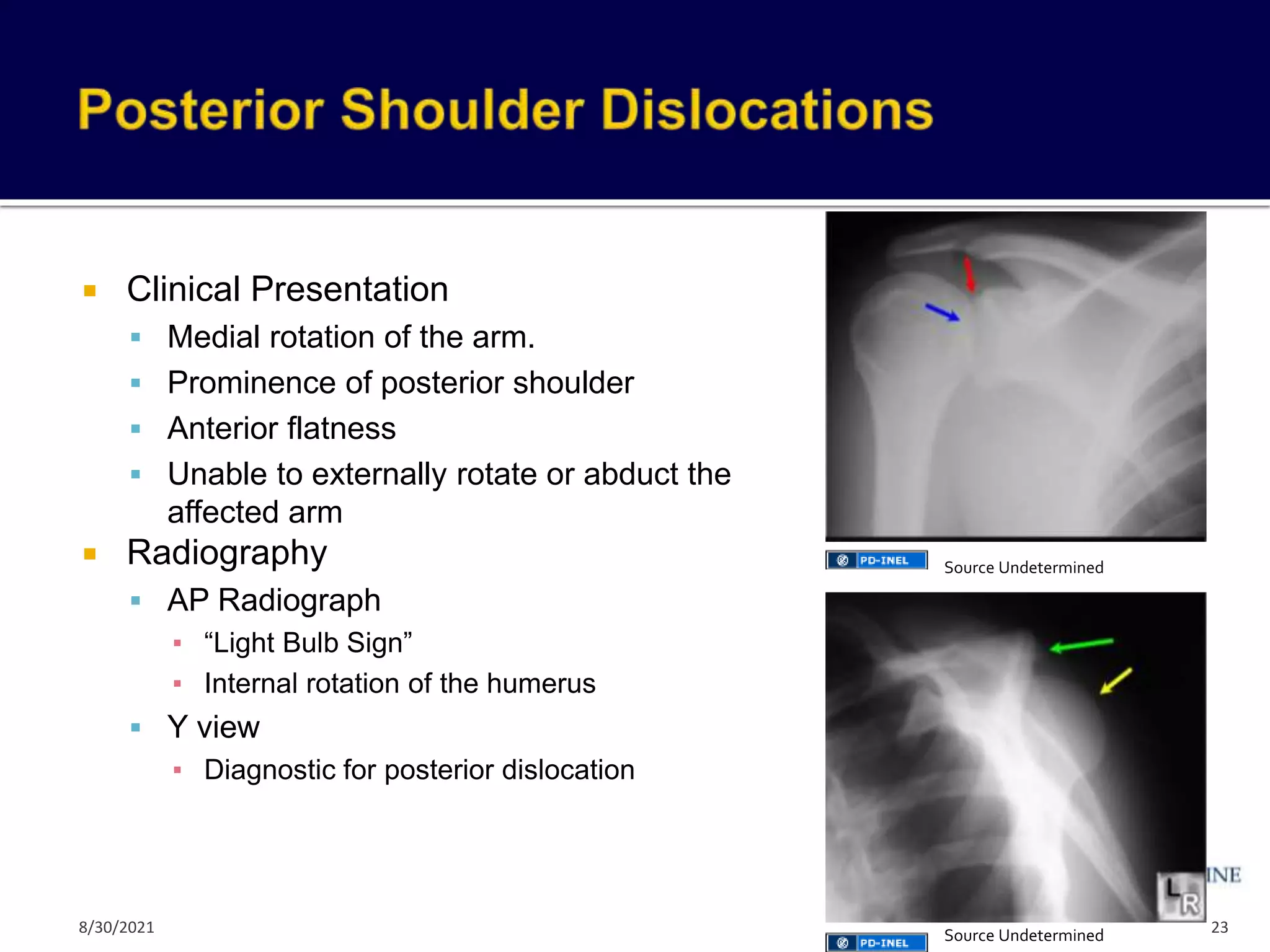
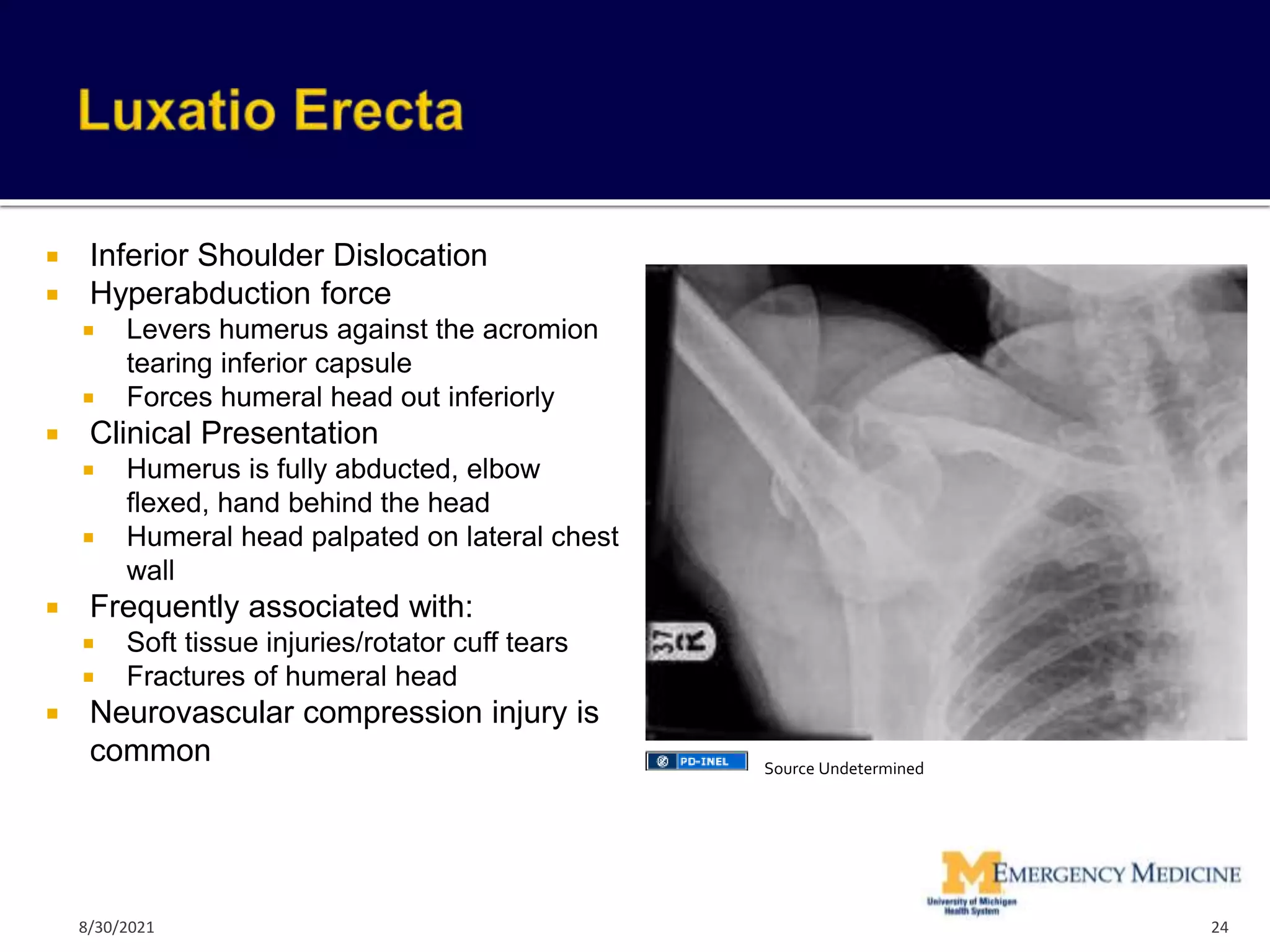
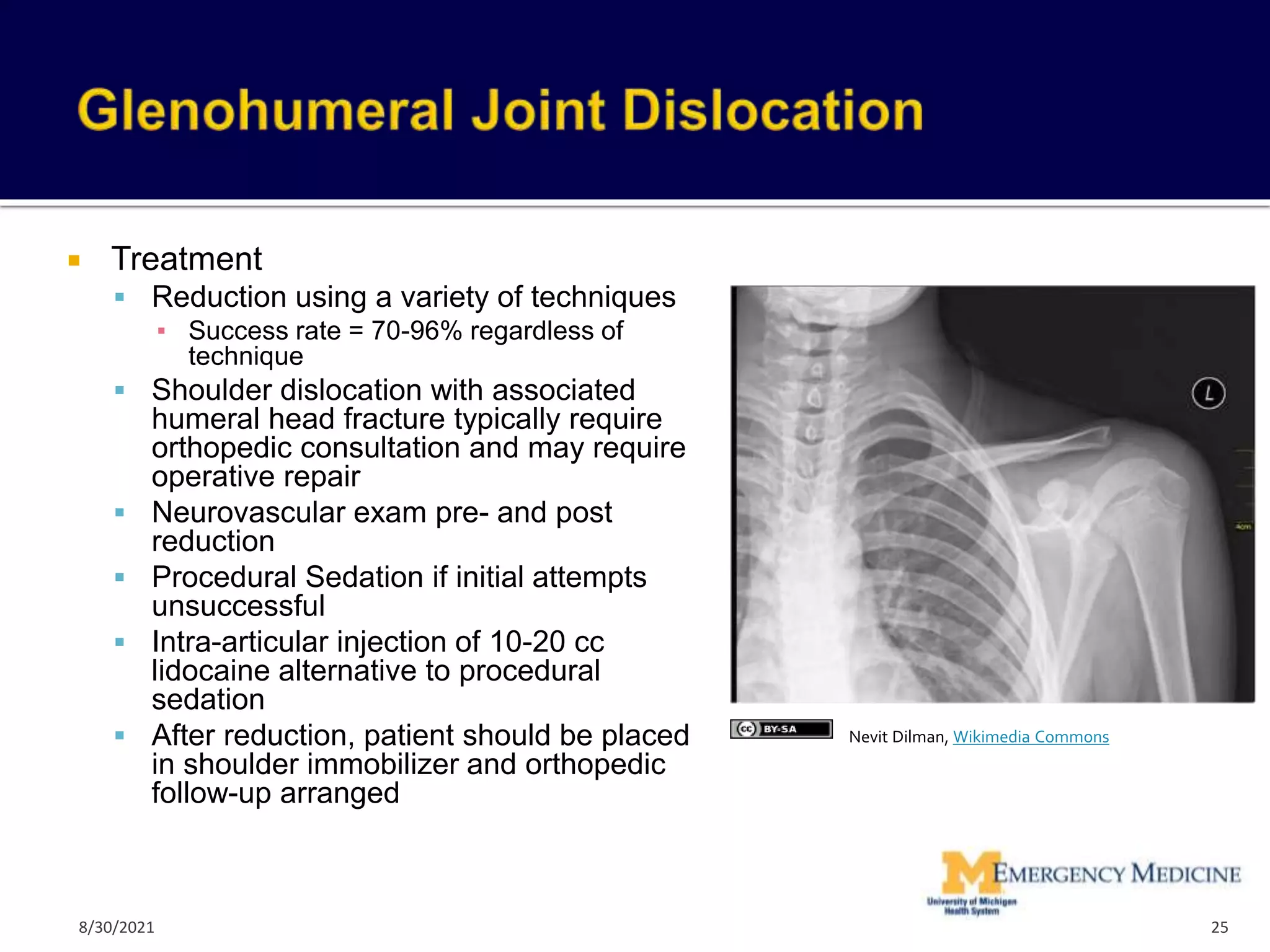
The document provides an overview of orthopedic injuries of the upper extremity, including the shoulder, arm, elbow, forearm, and wrist. It reviews common fractures and dislocations, their presentations, diagnostic approaches, and treatment options. Key injuries discussed include sternoclavicular dislocations, acromioclavicular separations, clavicle and scapula fractures, and shoulder dislocations.