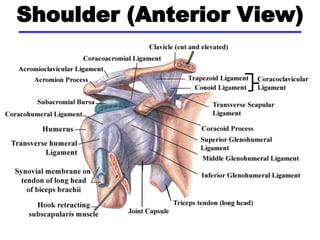
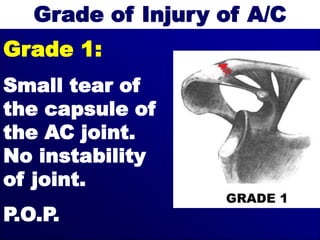
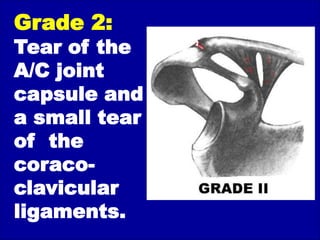
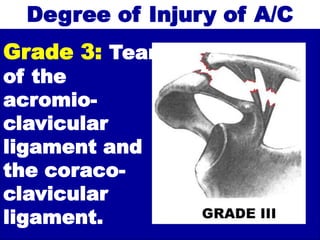
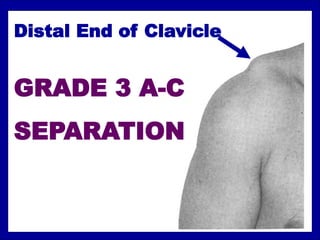
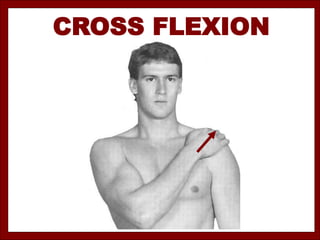
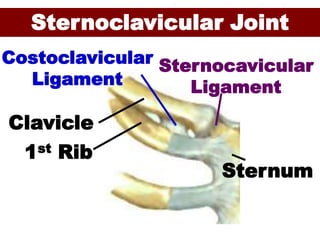
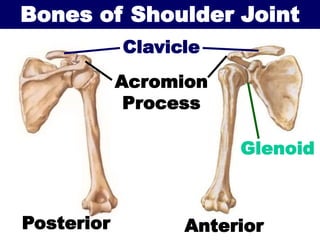
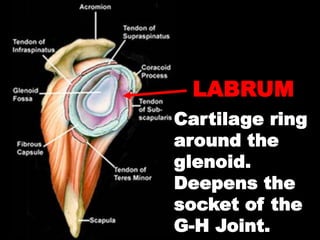
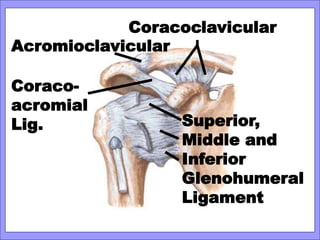
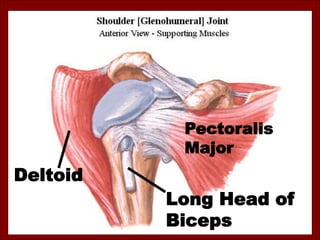
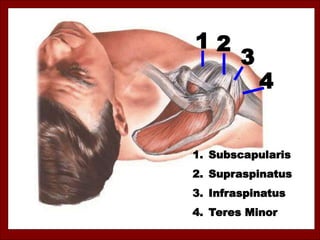
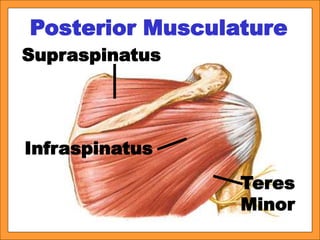
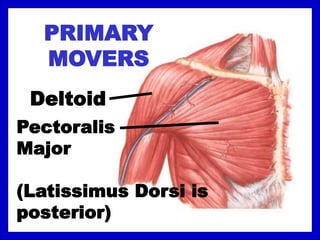
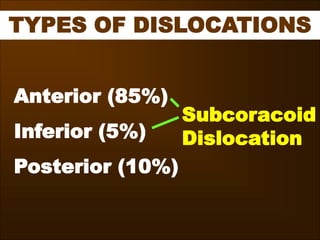
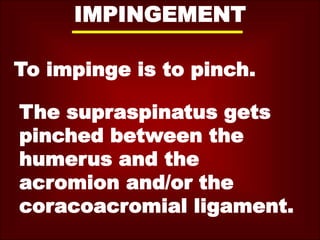
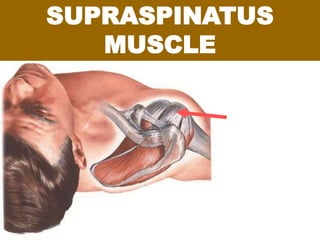
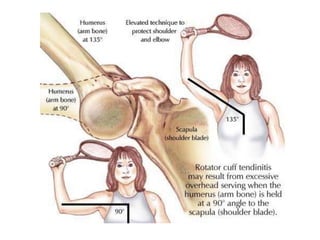
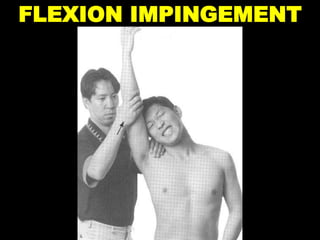
This document discusses various injuries and conditions related to the shoulder. It covers topics like shoulder anatomy, types of separations and fractures, mechanisms of different injuries, grades of injuries, signs and symptoms, treatment approaches, and more. Specific conditions covered include acromioclavicular separations, clavicle fractures, sternoclavicular joint separations, shoulder dislocations, supraspinatus tendonitis, and impingement syndrome. Diagrams are included to illustrate shoulder anatomy and various injuries.