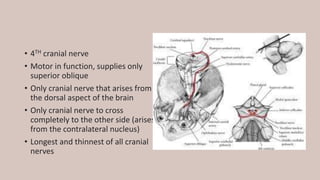
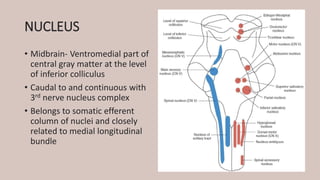
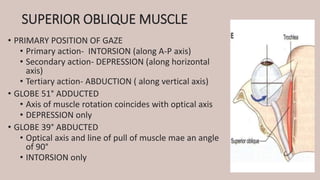
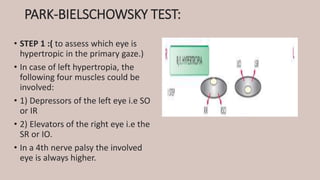
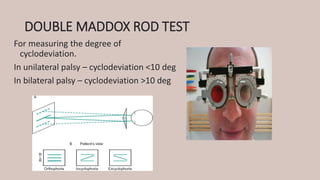
The trochlear nerve is the 4th cranial nerve that innervates the superior oblique muscle. It arises from the midbrain and is the only cranial nerve that crosses sides completely. Damage to the trochlear nerve causes weakness of the superior oblique muscle resulting in vertical diplopia that is worse on downward gaze and head tilt toward the affected side. The Park-Bielschowsky test can help localize the cause of vertical strabismus to the superior oblique muscle. Treatment depends on the severity and may include prisms, muscle surgery, or tendon procedures.