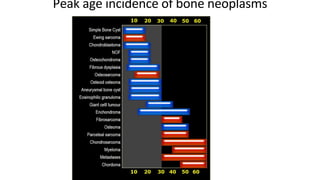
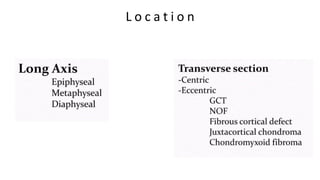
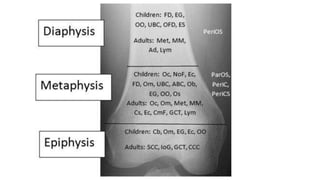
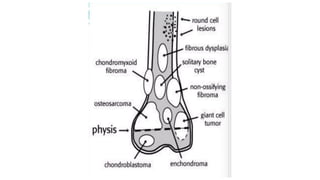
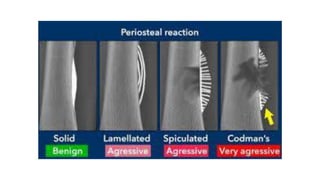
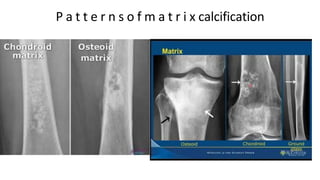
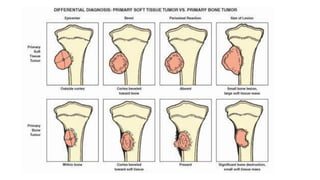
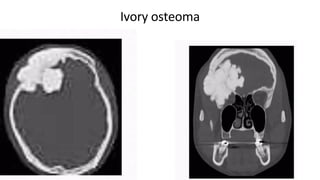
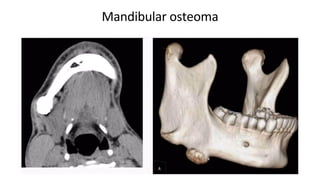
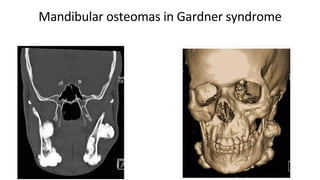
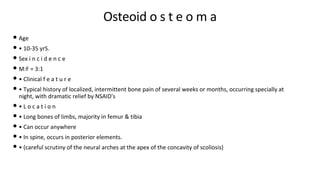
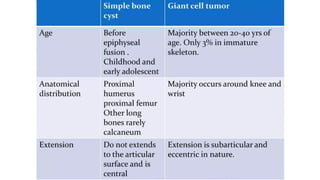
The document discusses benign bone lesions, their classifications, diagnostic modalities, and imaging features. Various types of benign bone tumors are described, including osteoma, osteoid osteoma, chondromas, and fibrous tumors, each with specific characteristics regarding age incidence, location, and radiographic findings. It emphasizes the importance of imaging techniques like X-rays, CT scans, and MRIs for diagnosis and evaluation of these lesions.