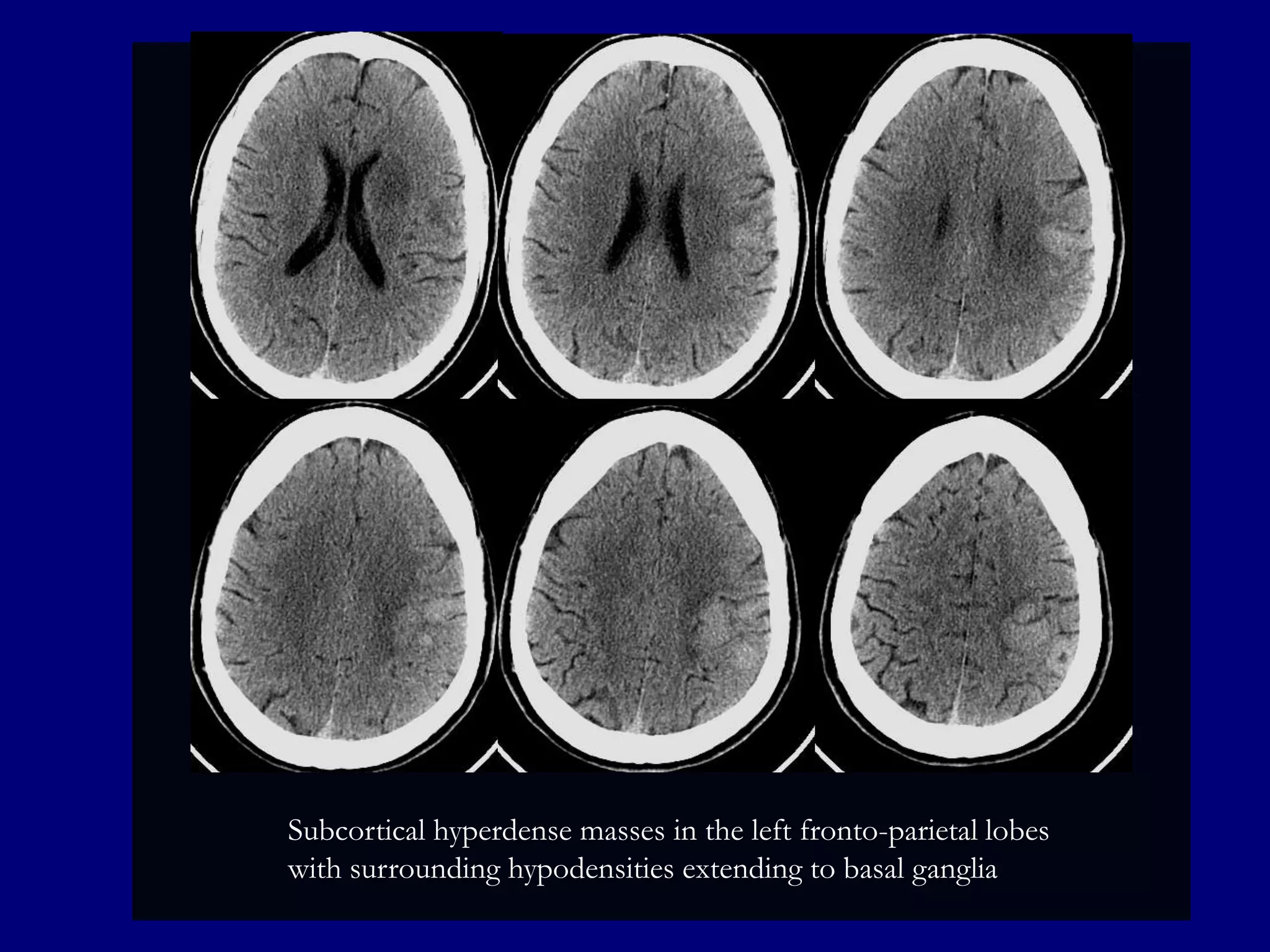
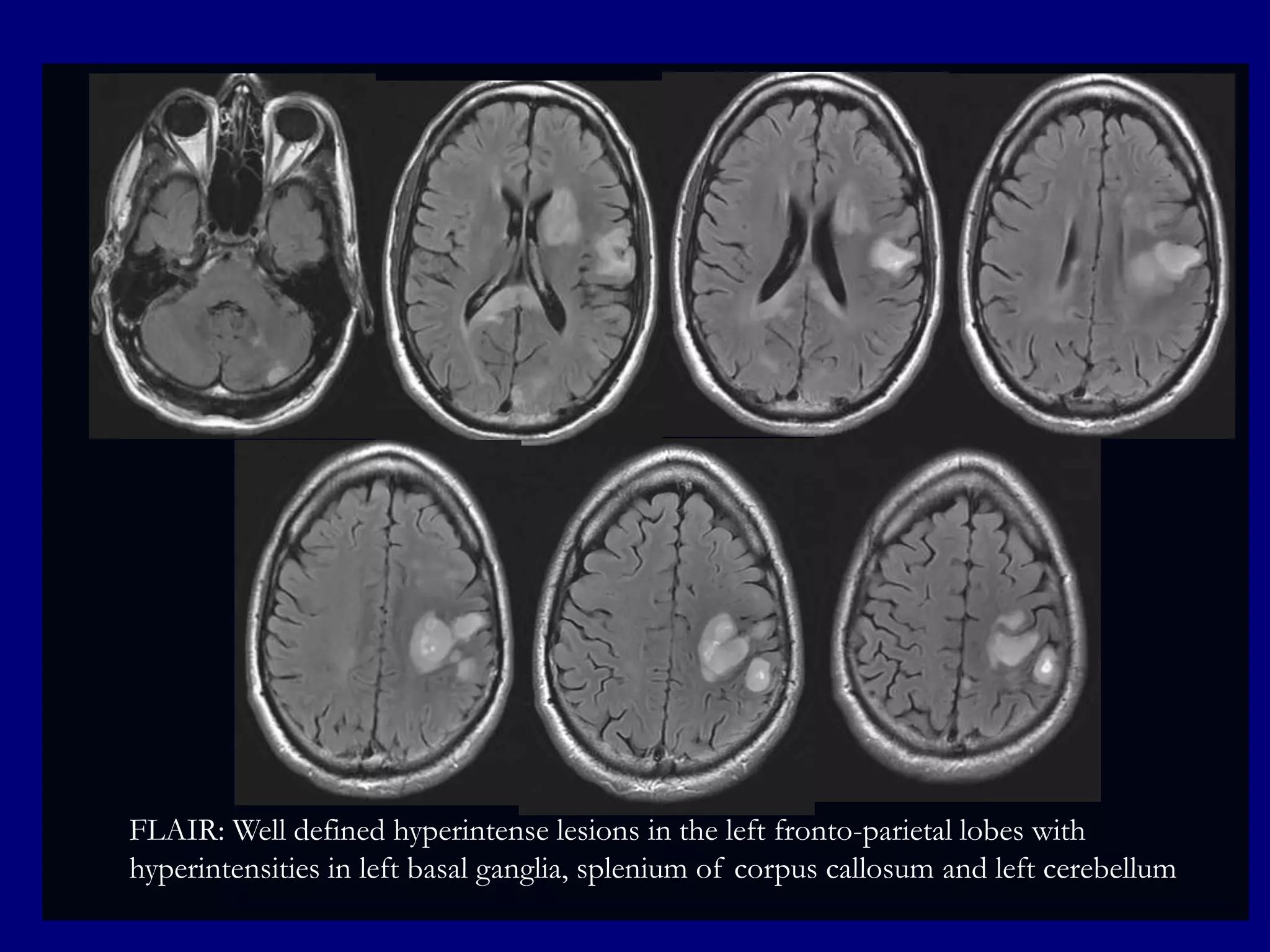
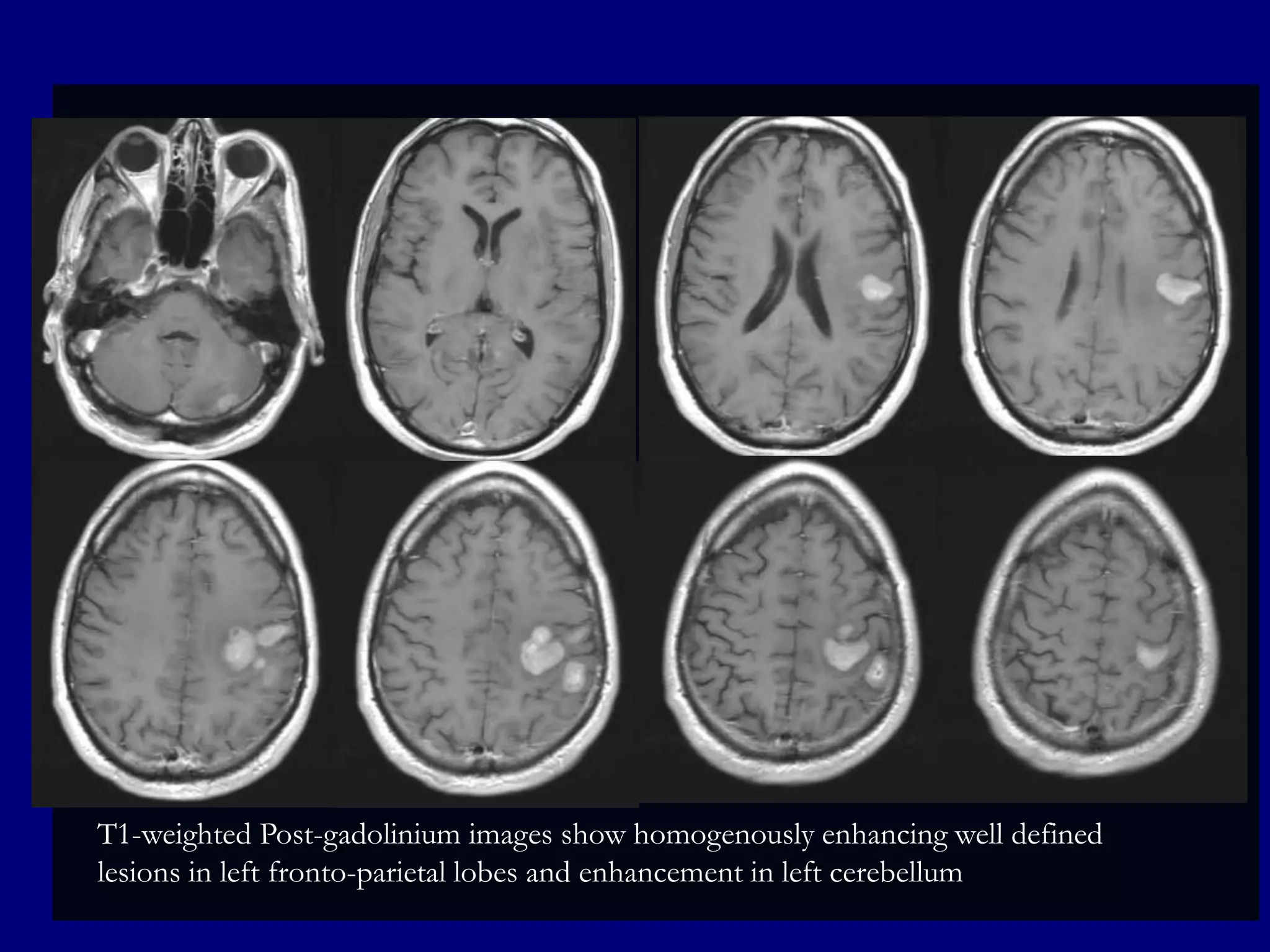
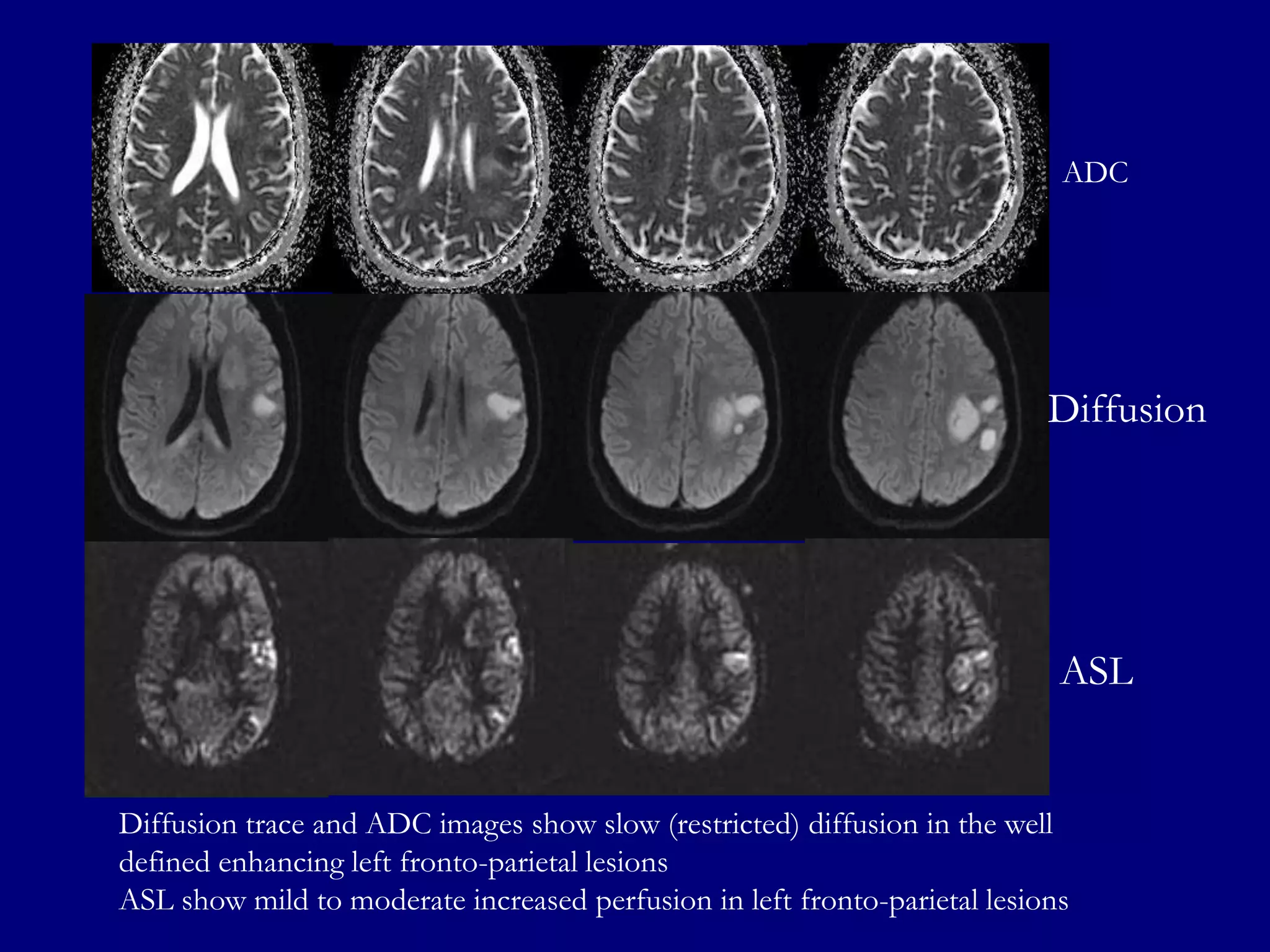
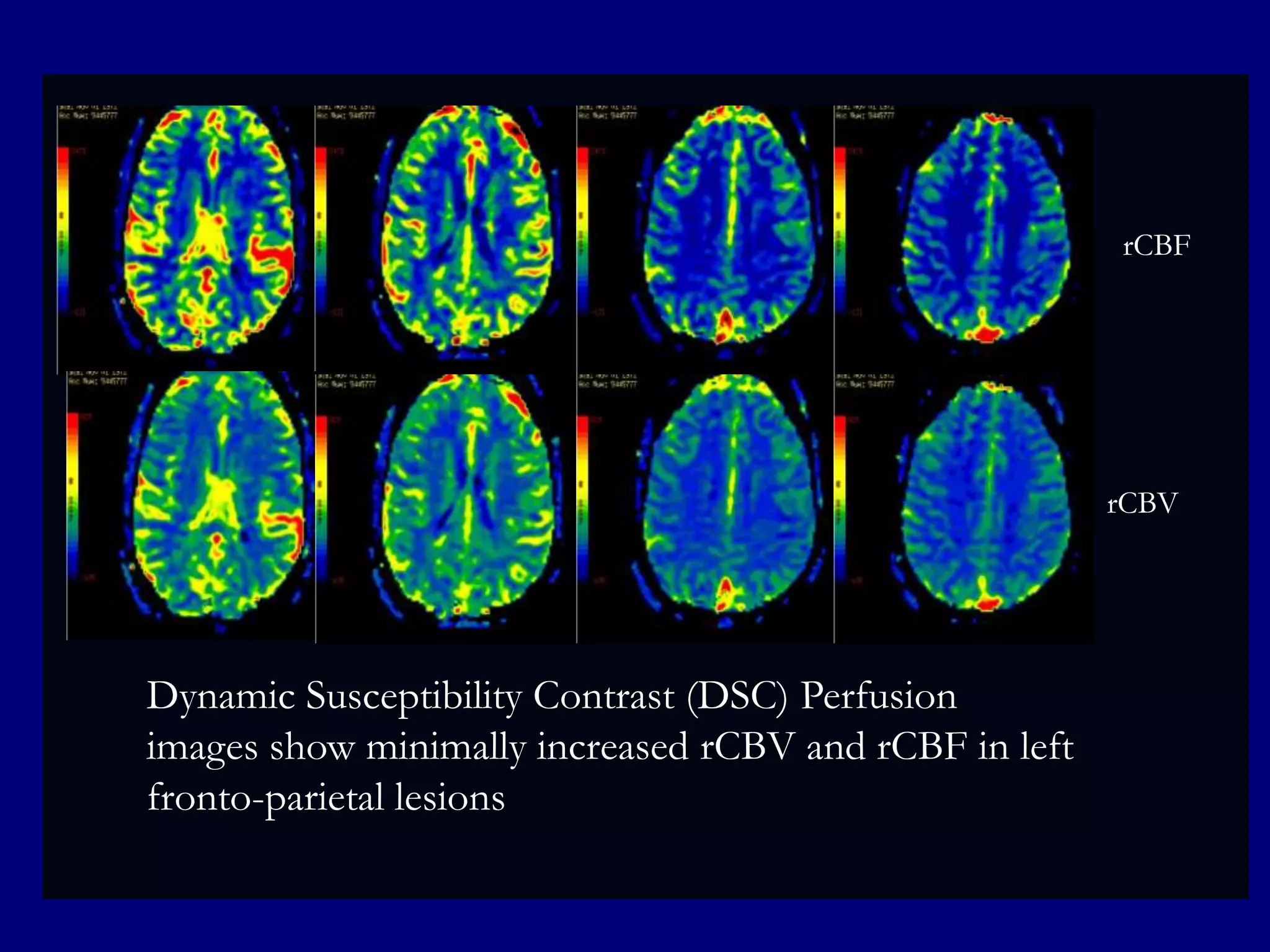
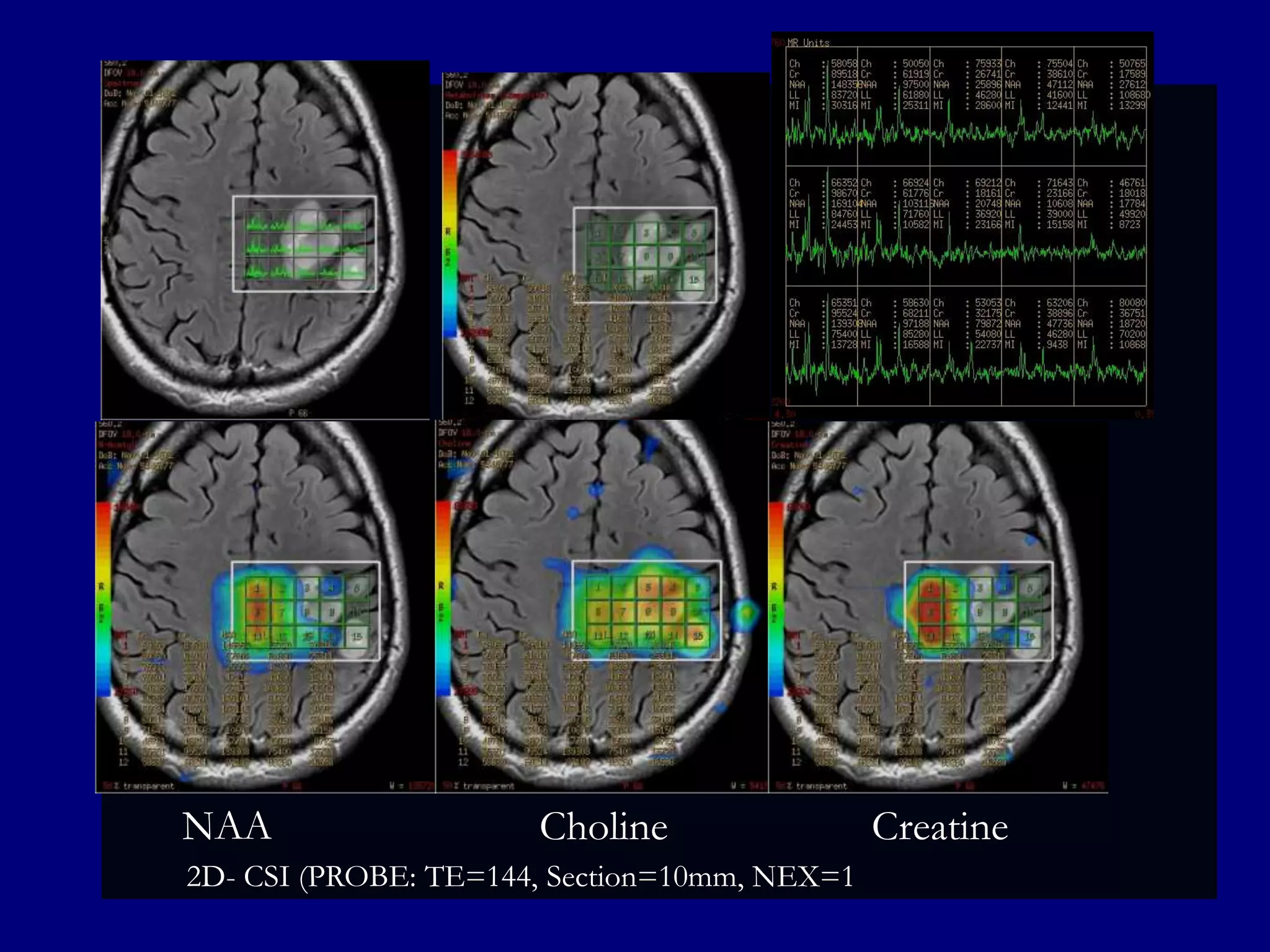
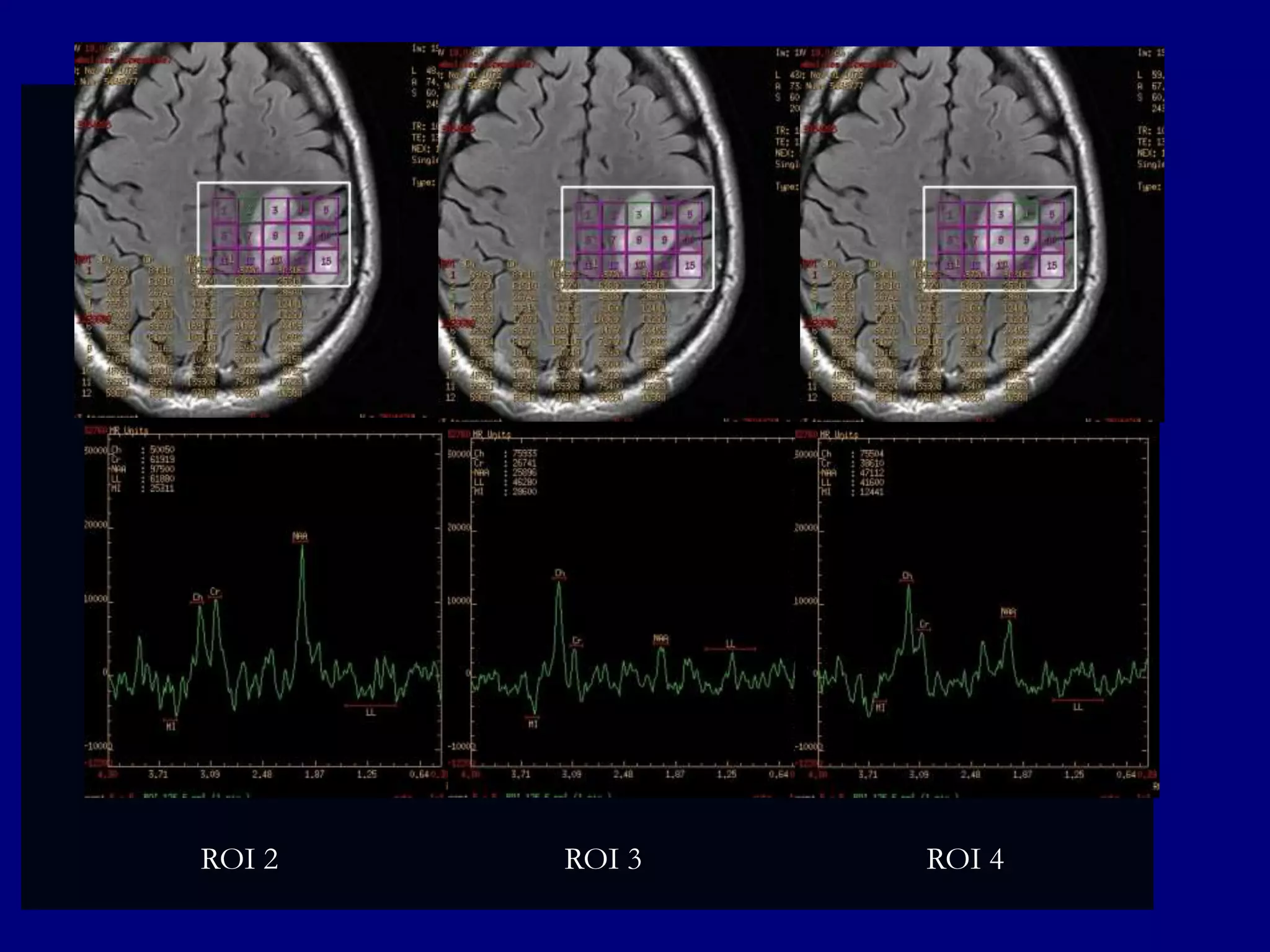
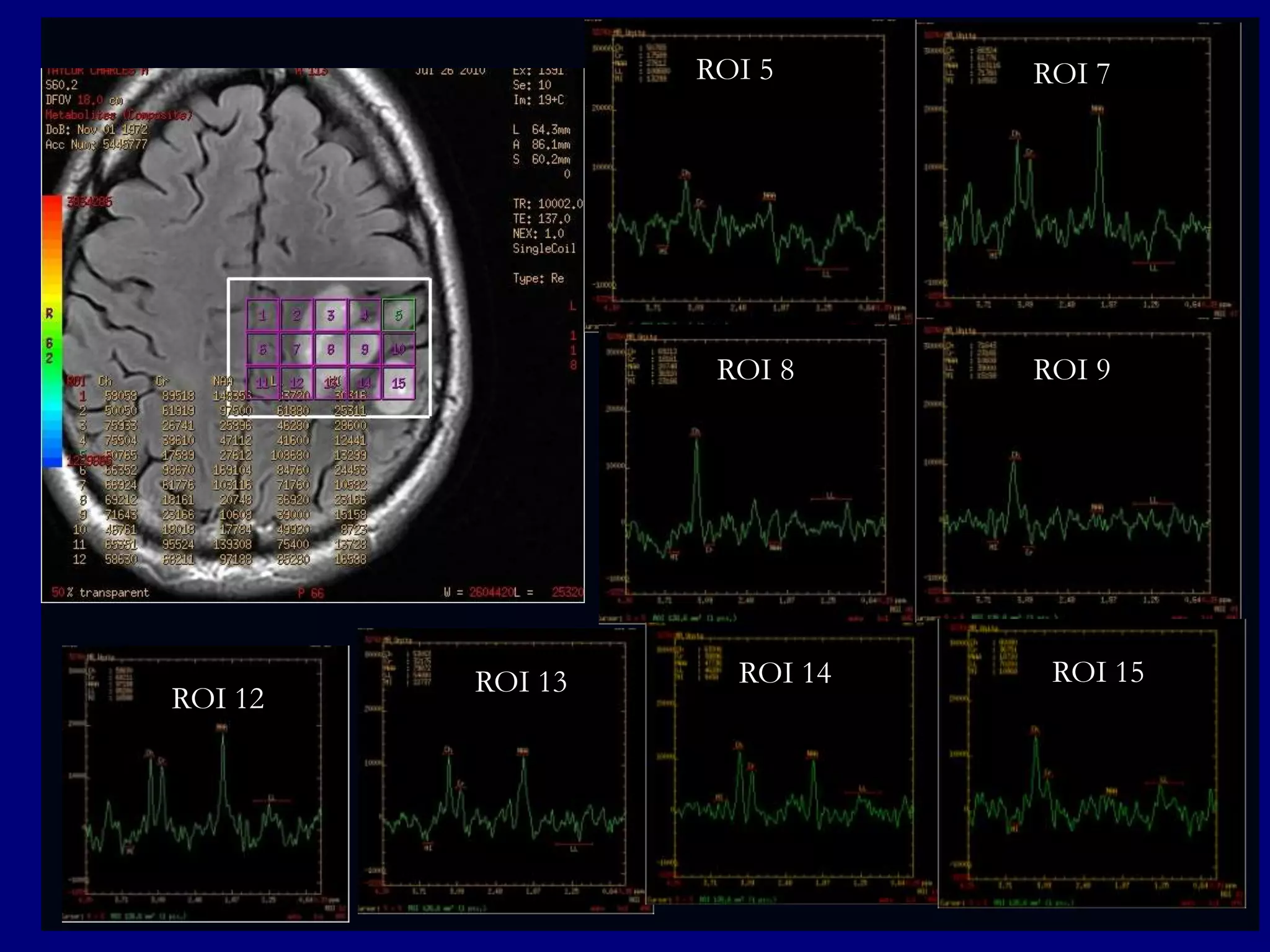
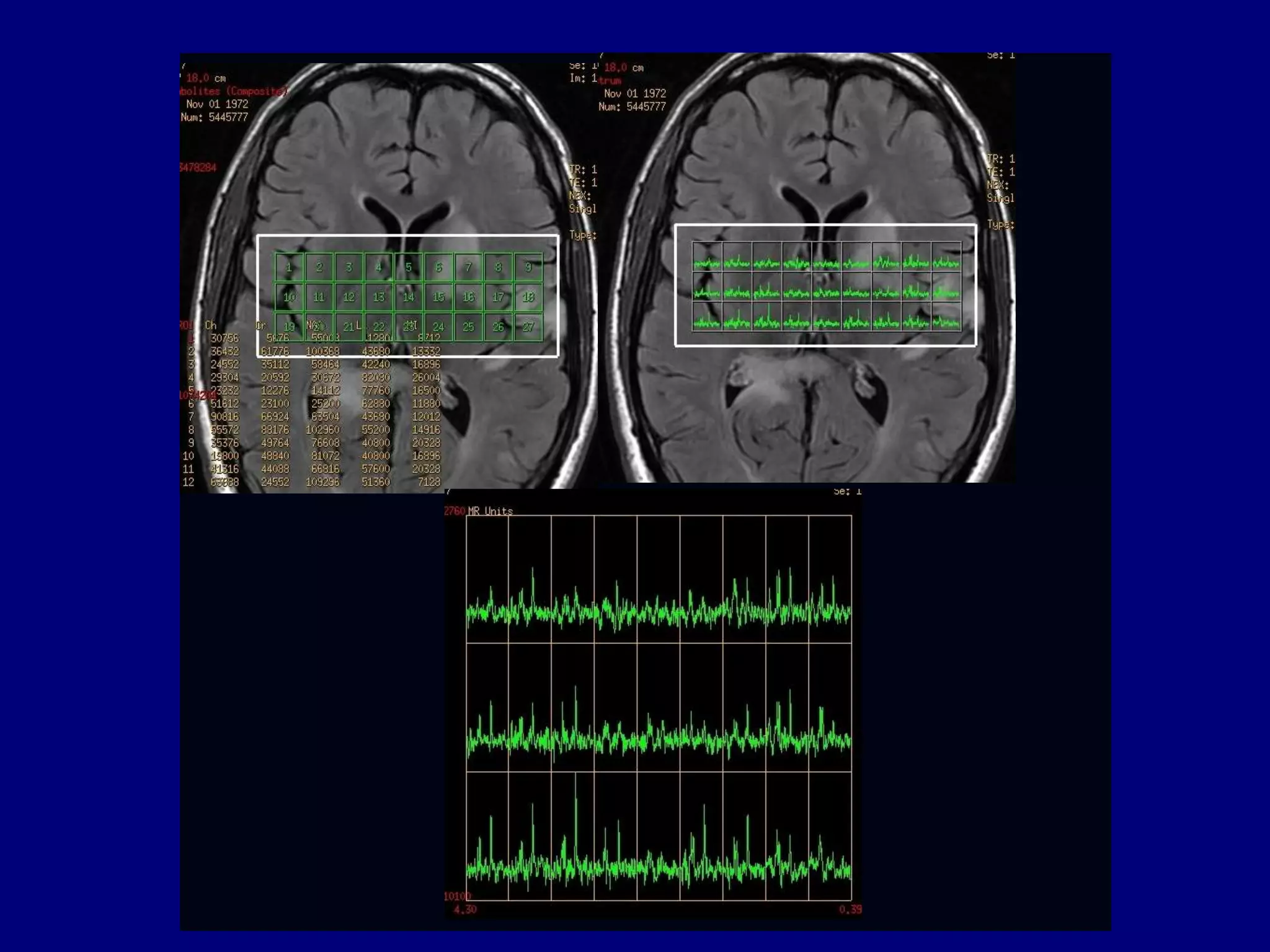
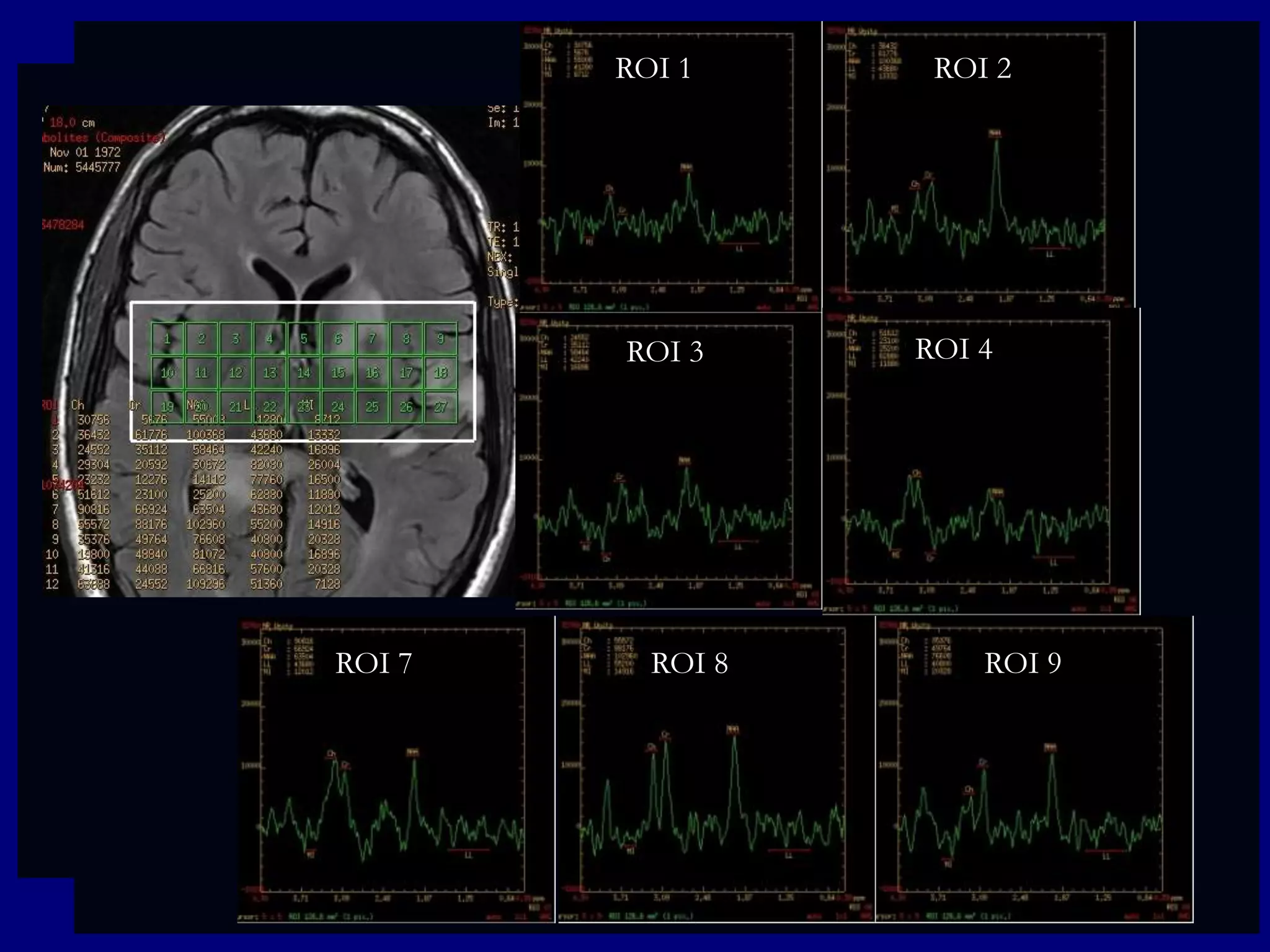
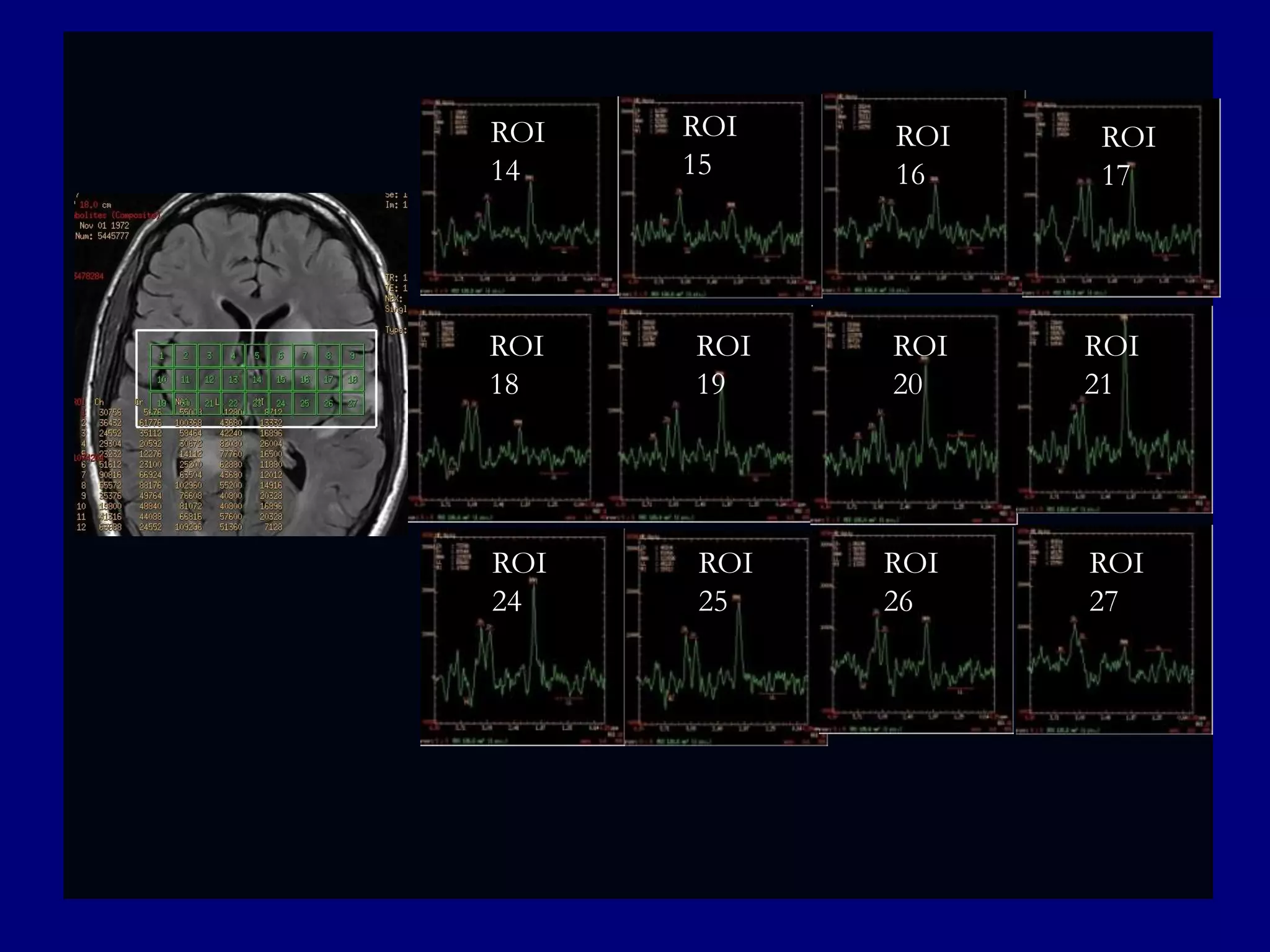
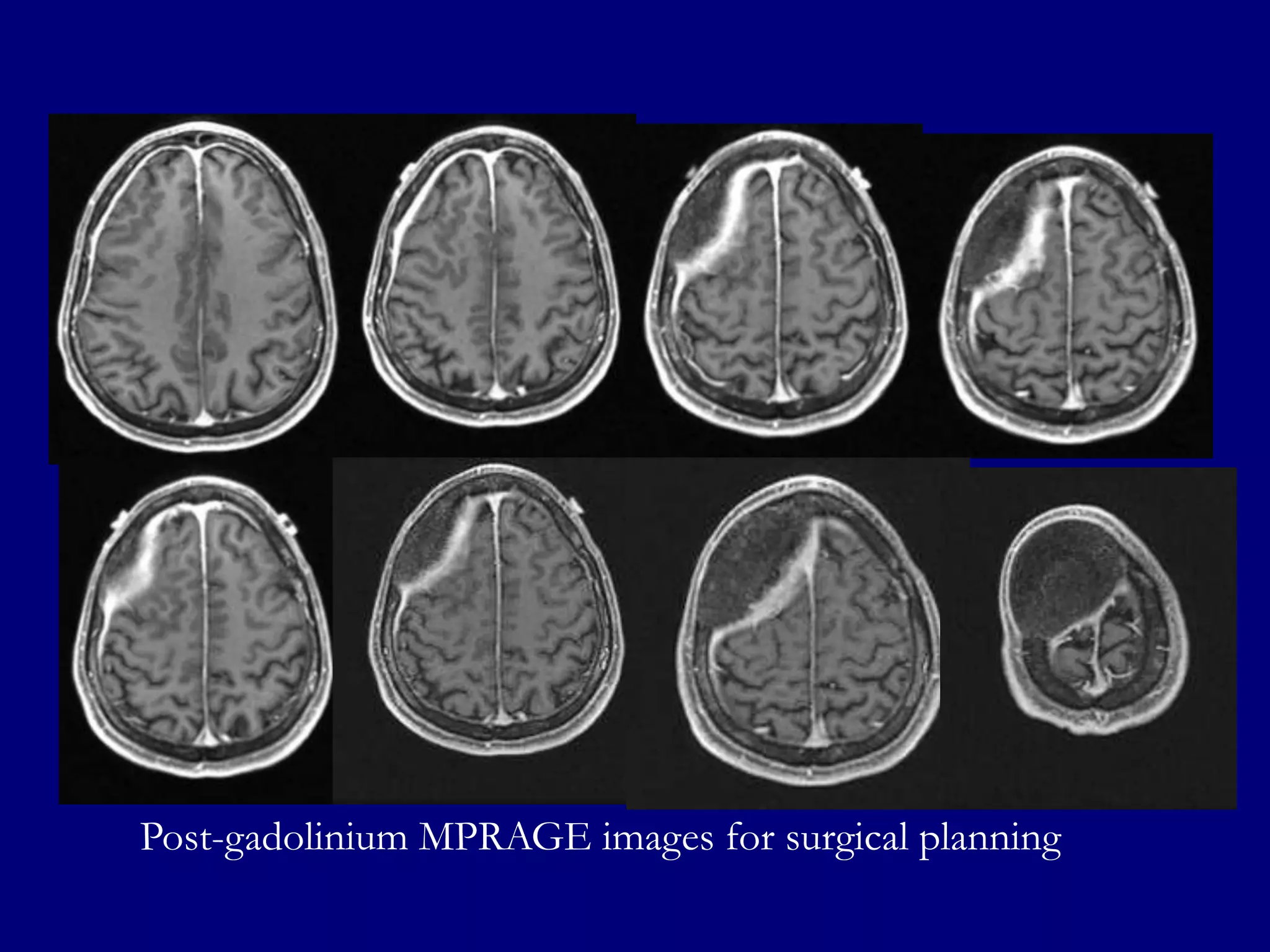
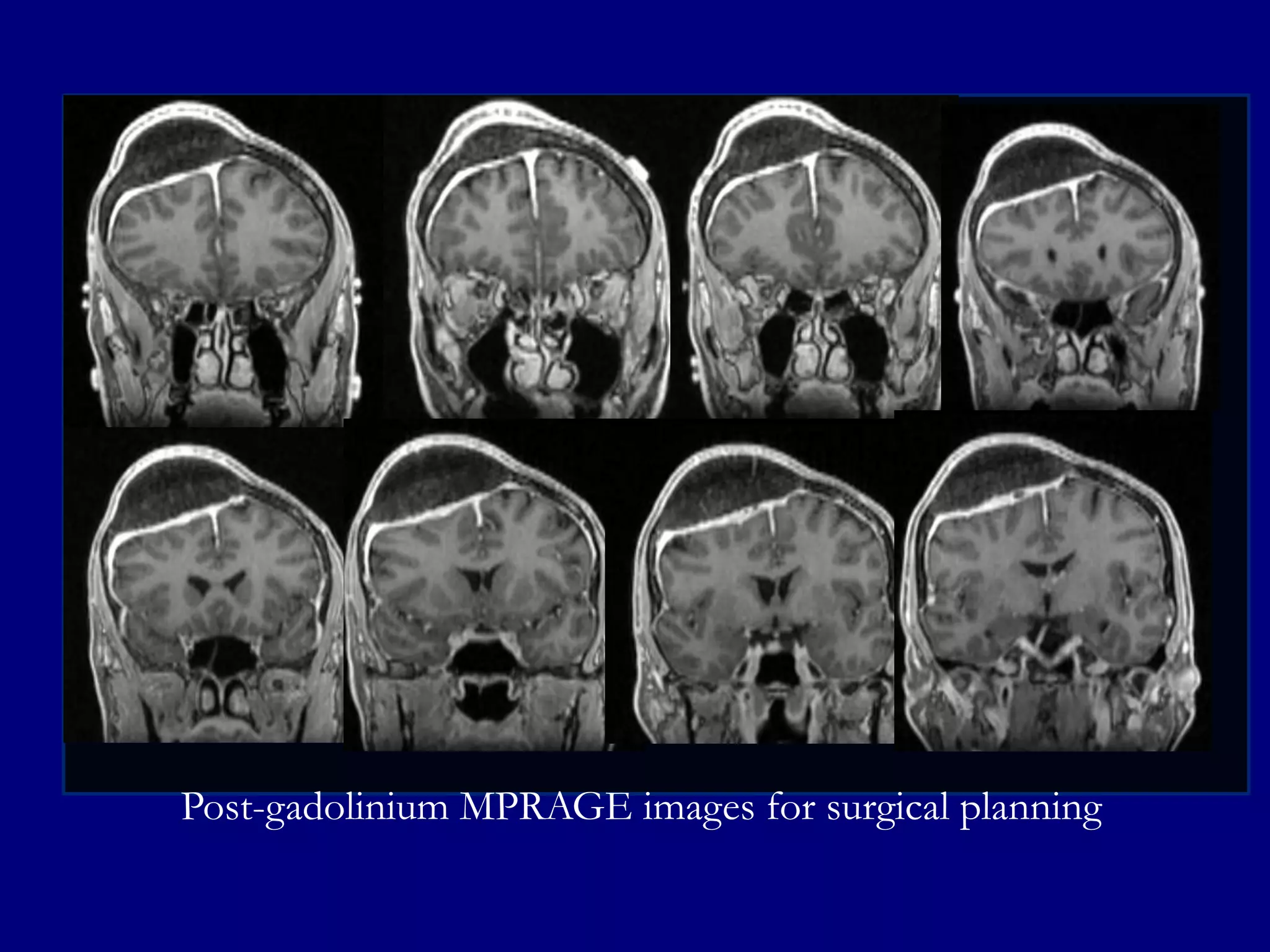
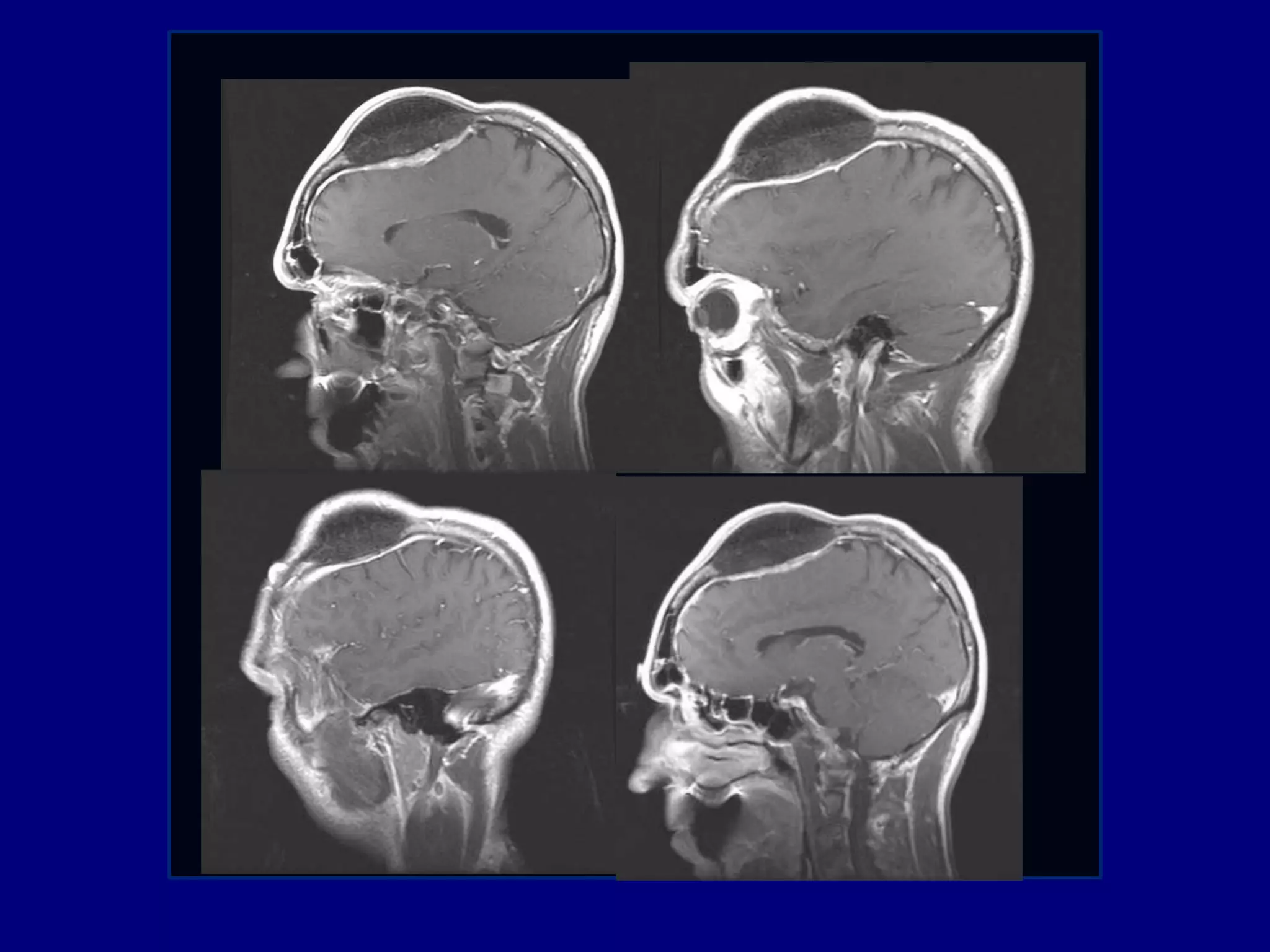
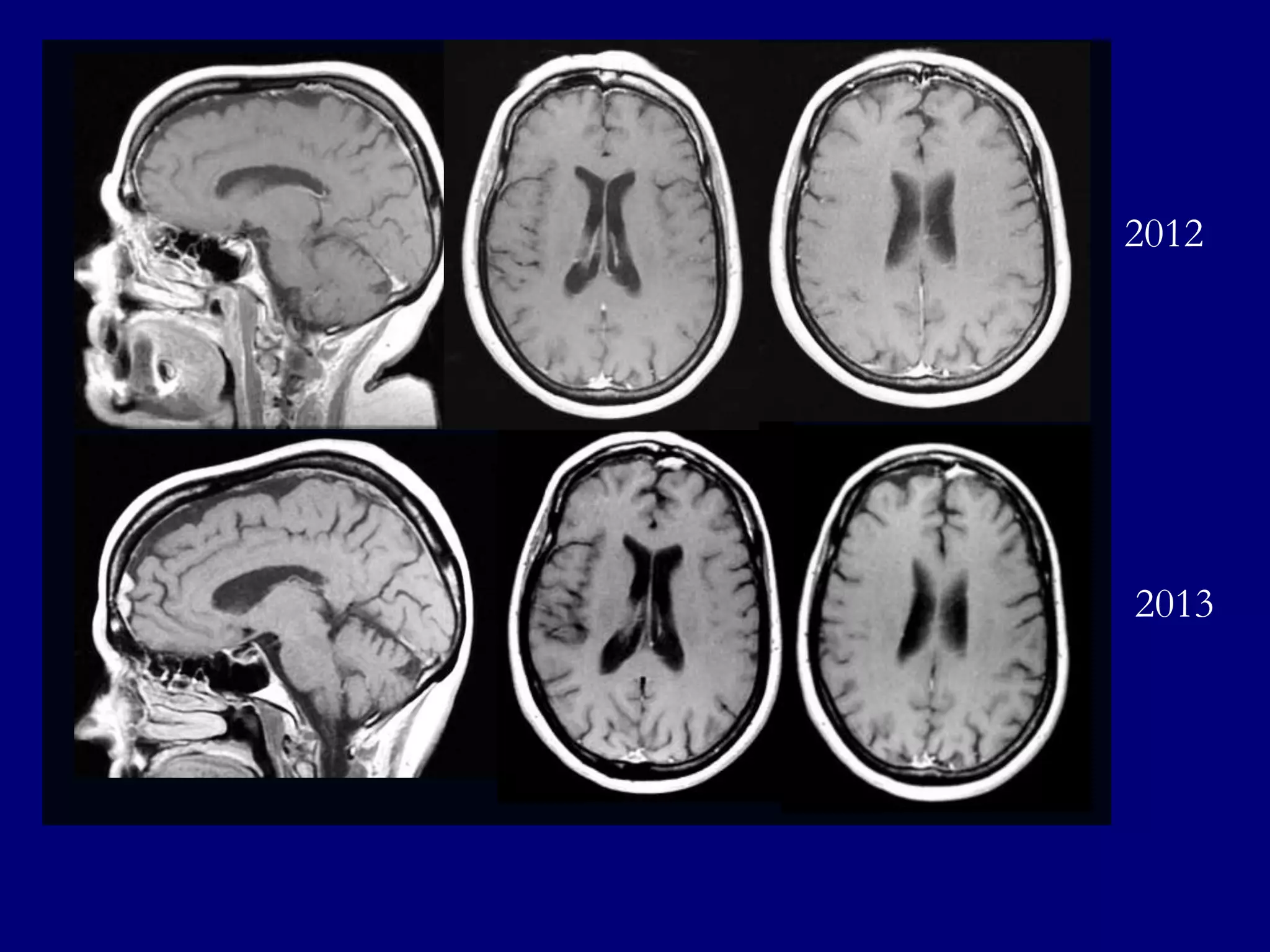
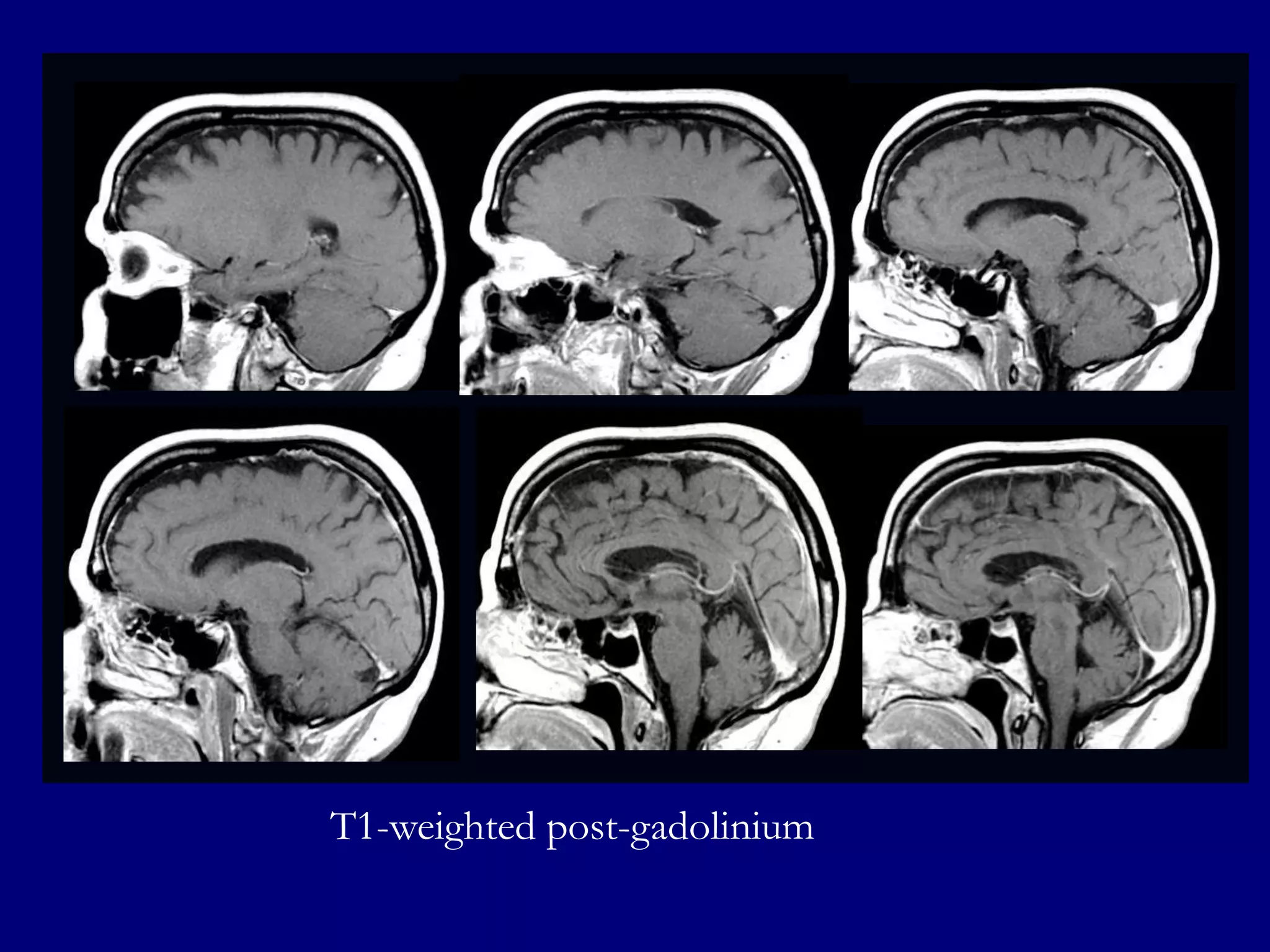
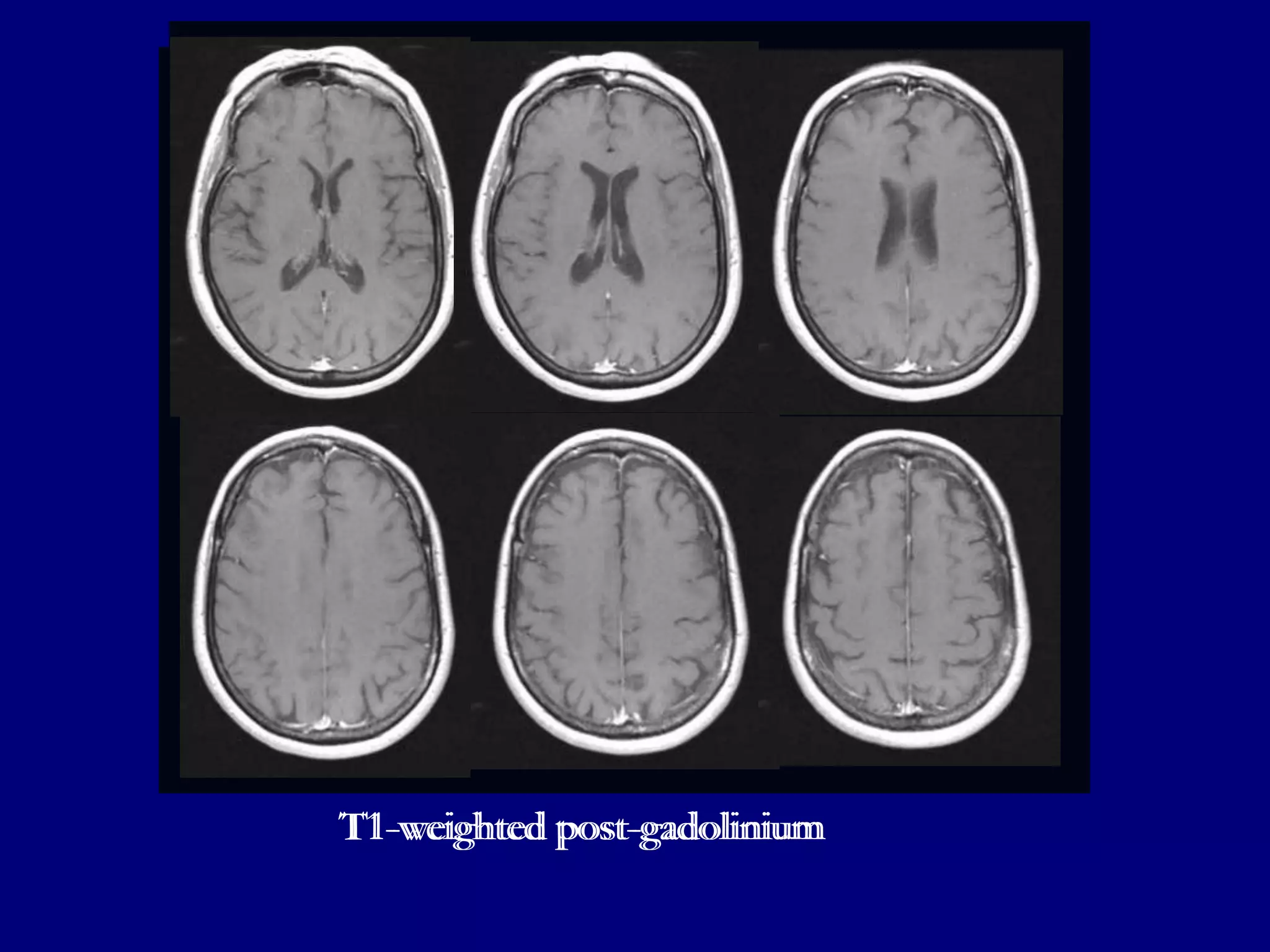
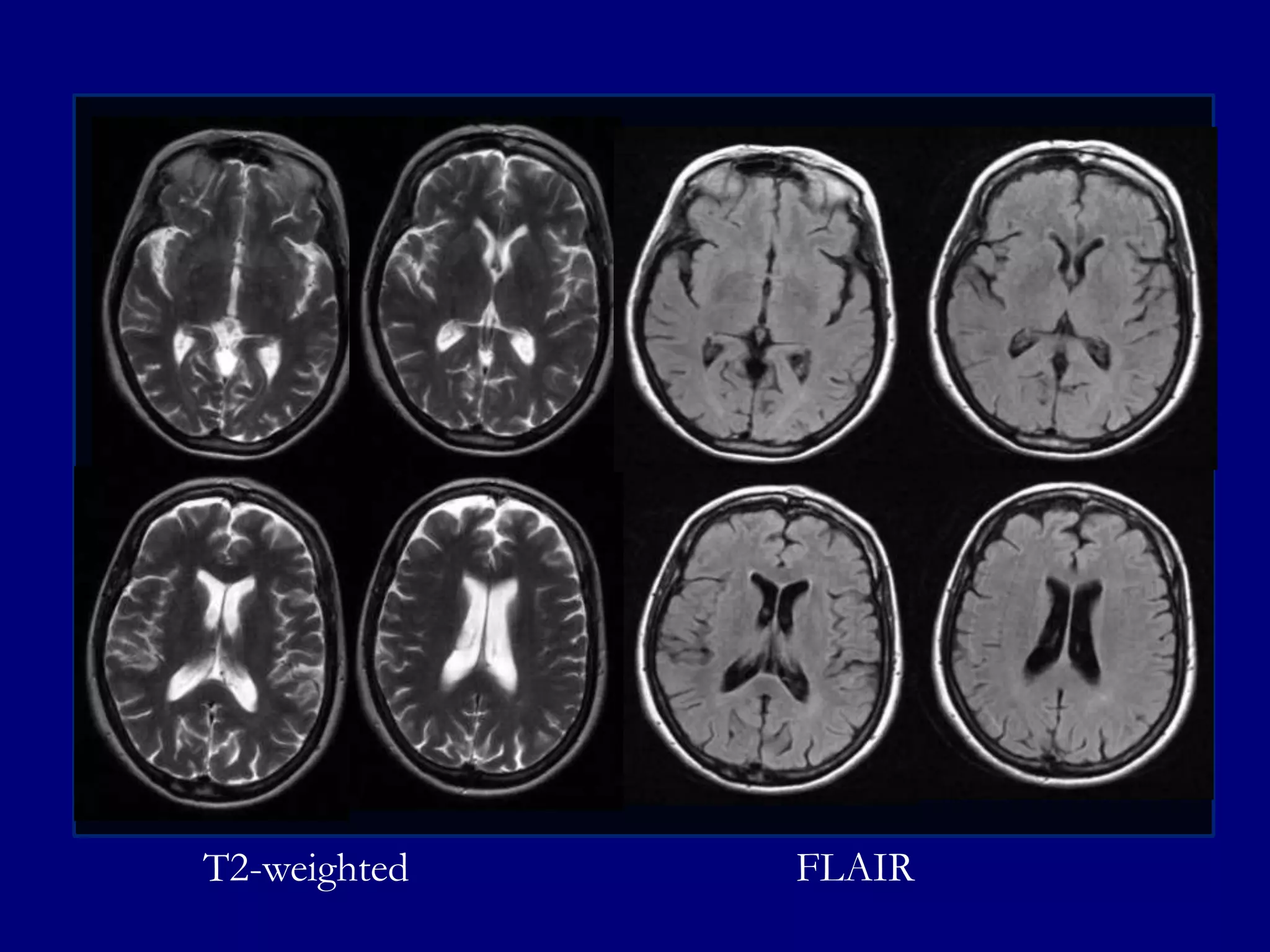
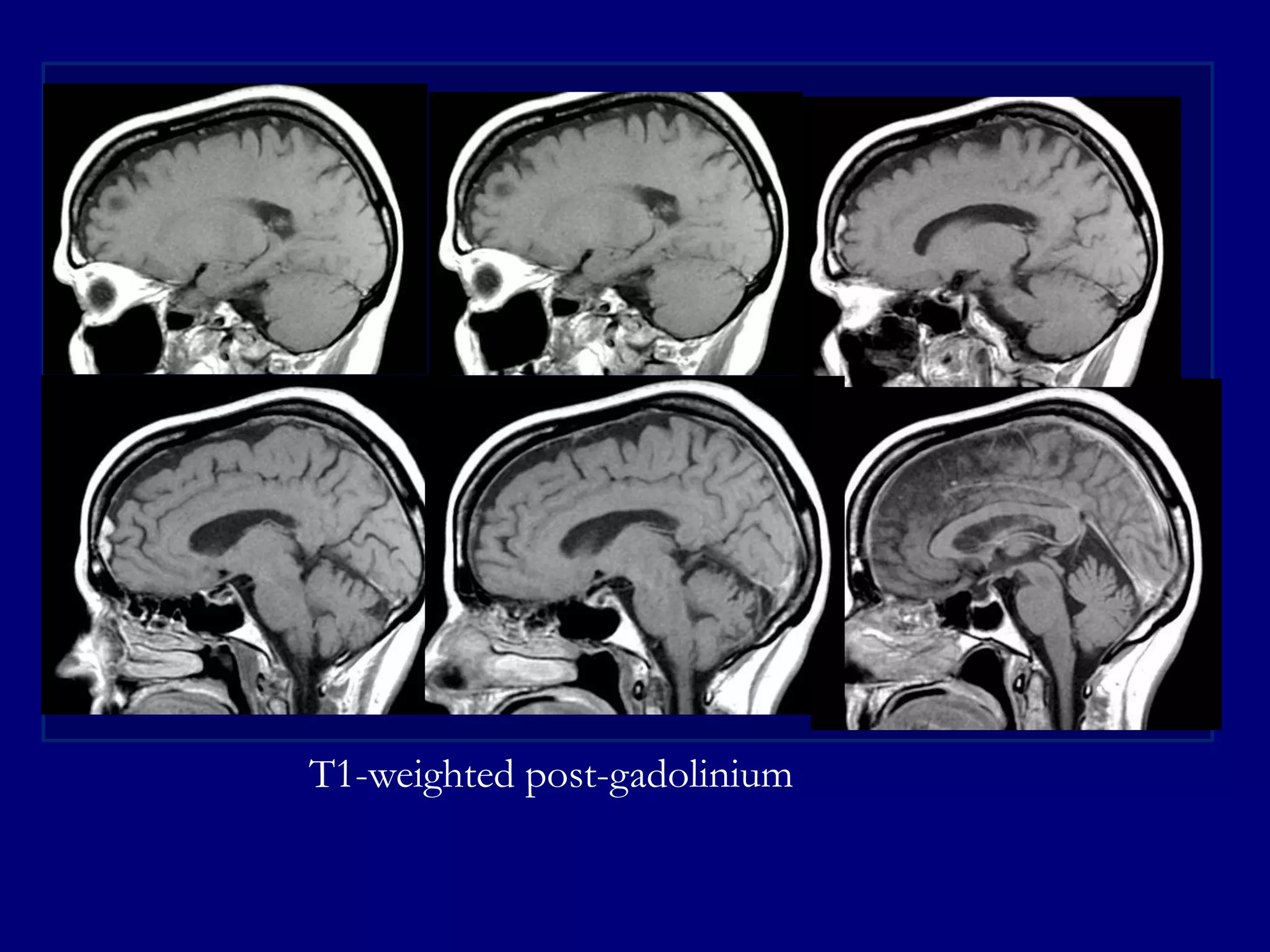
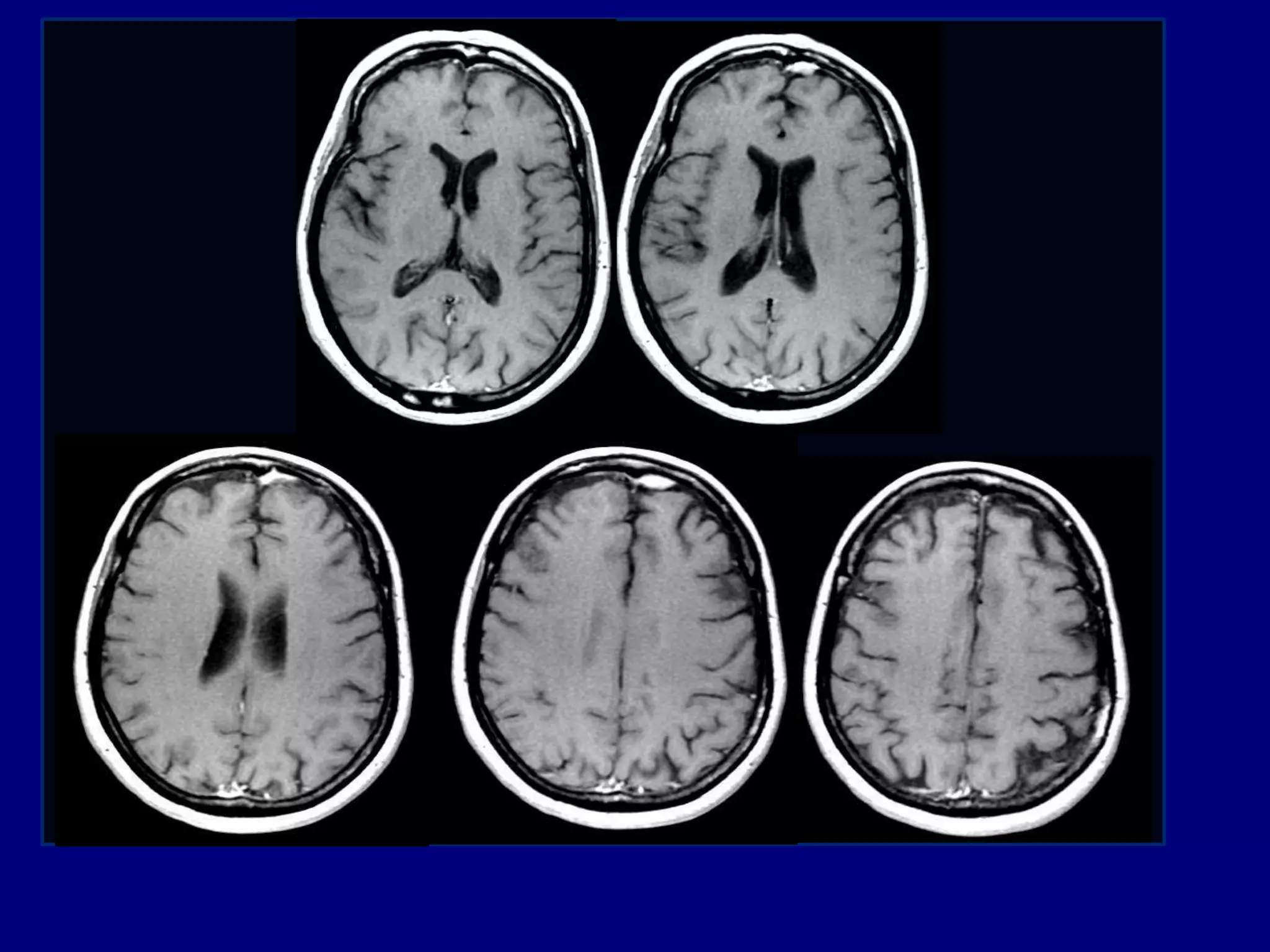
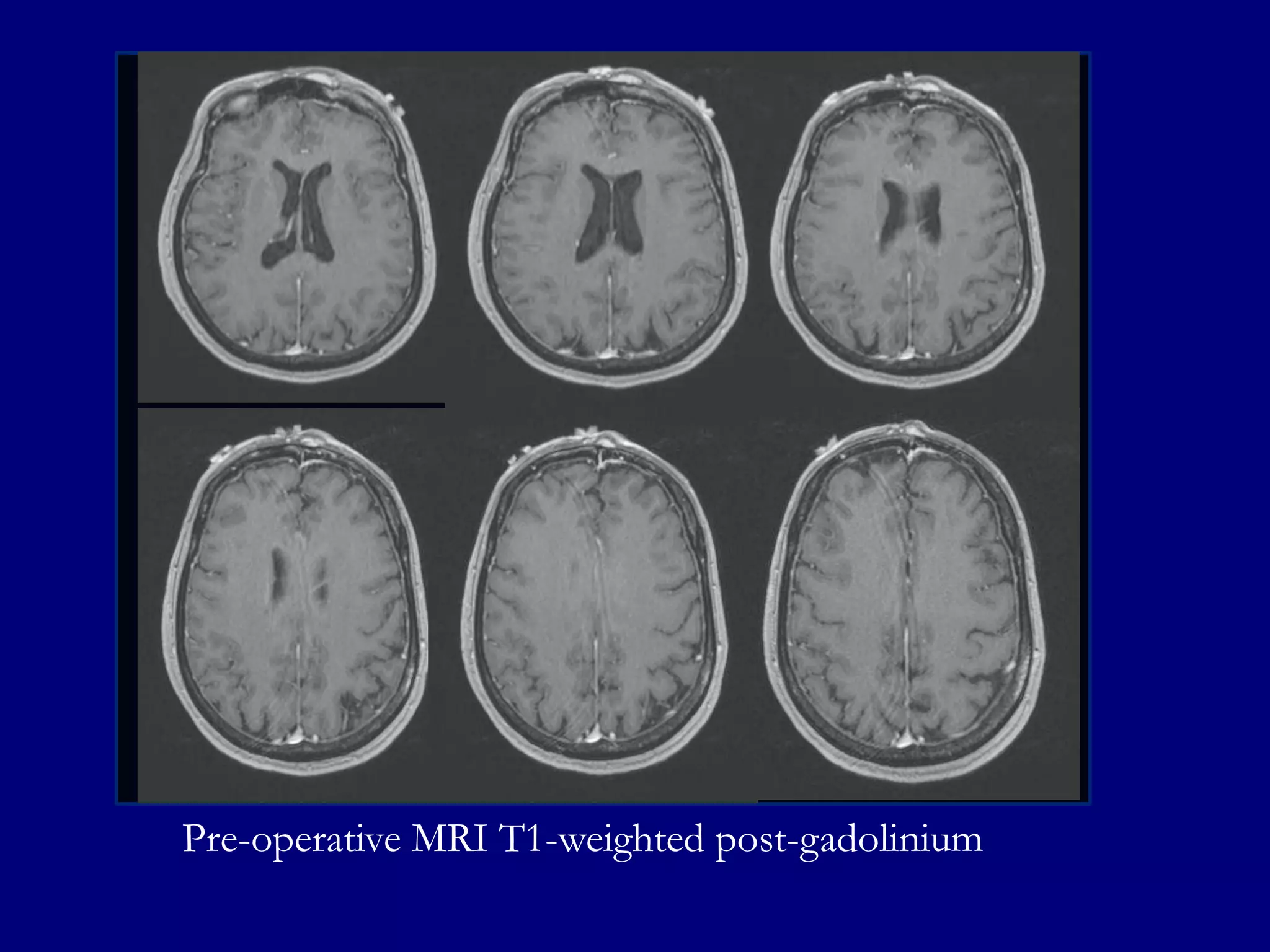
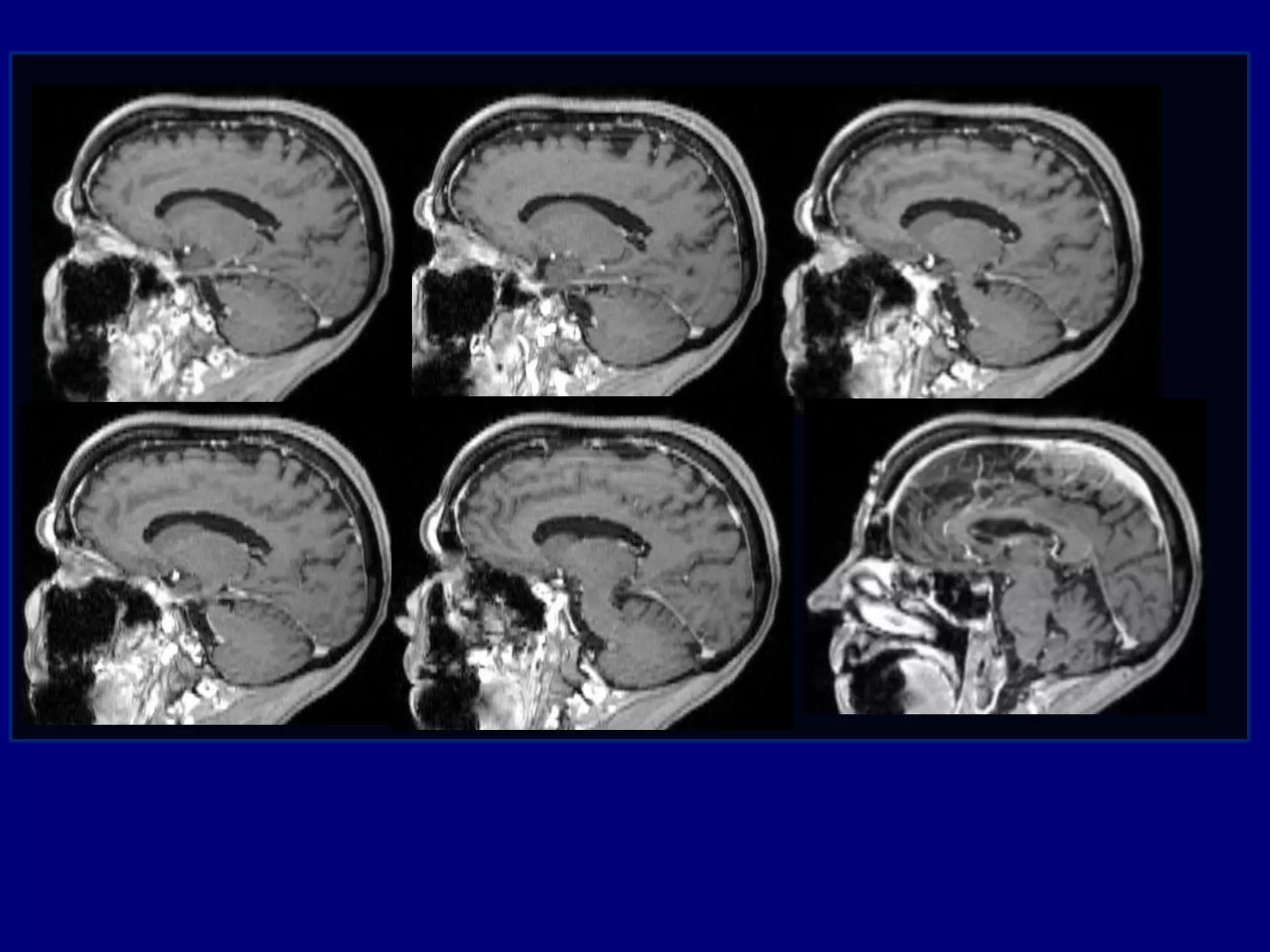
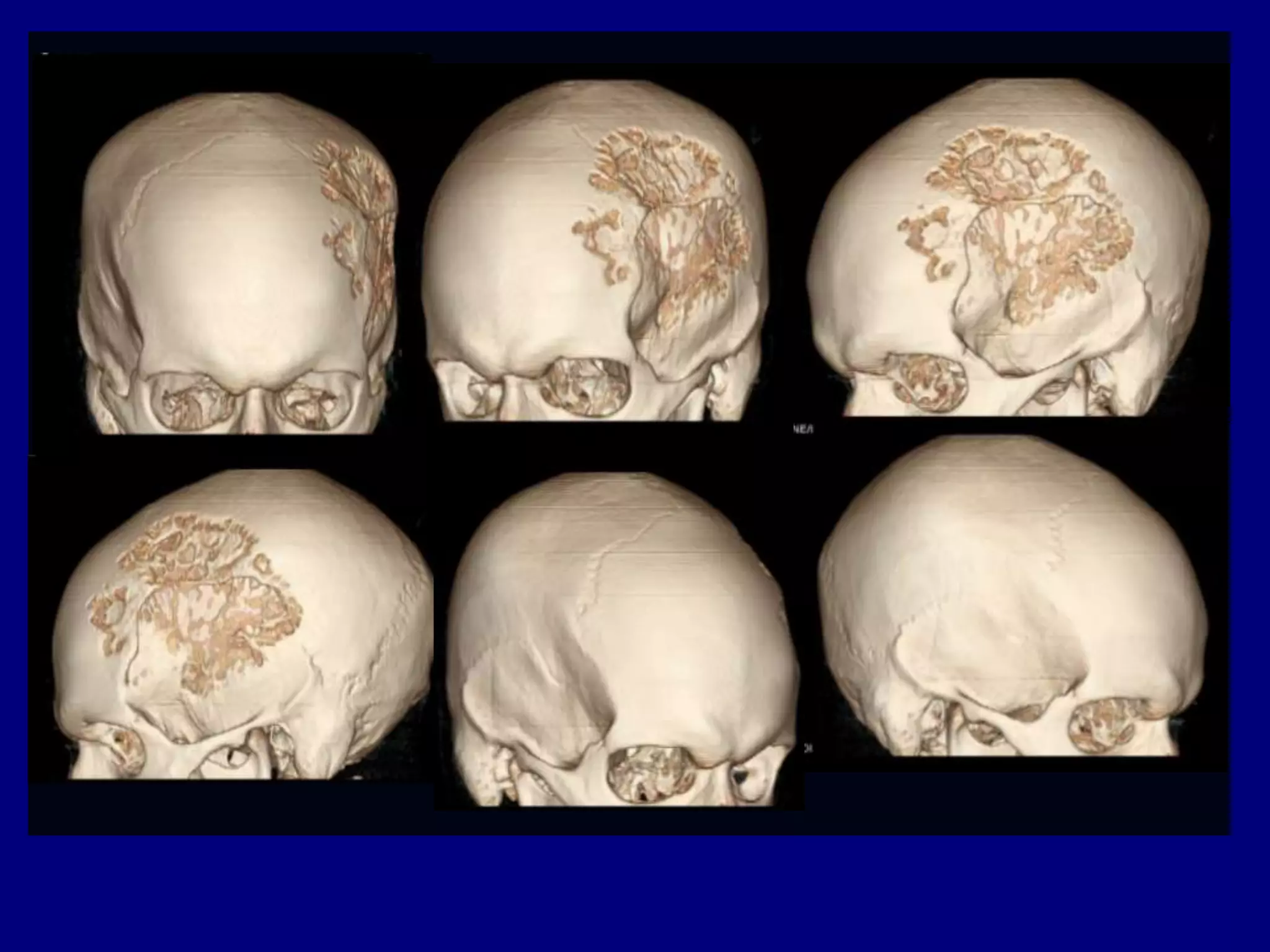
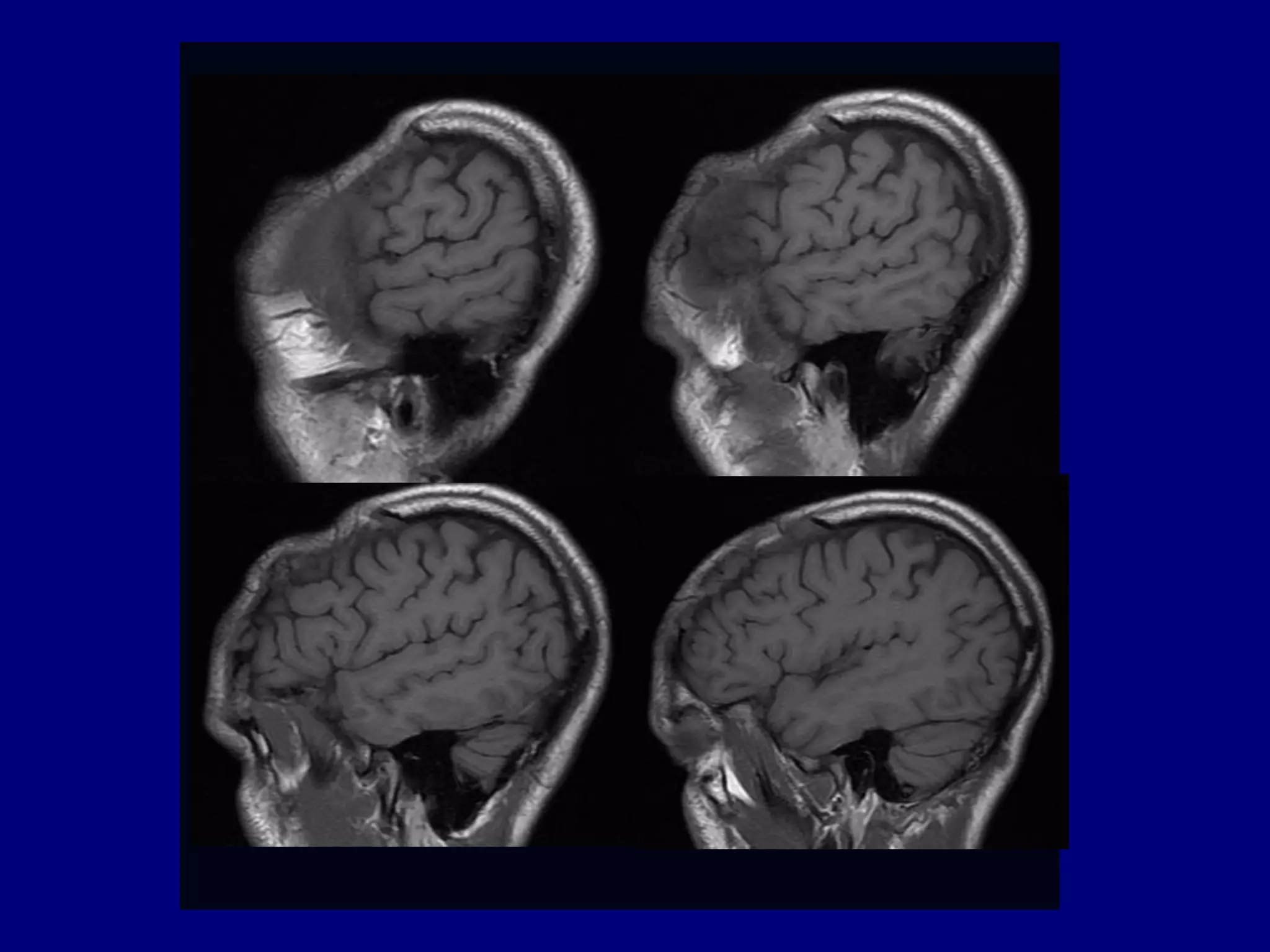
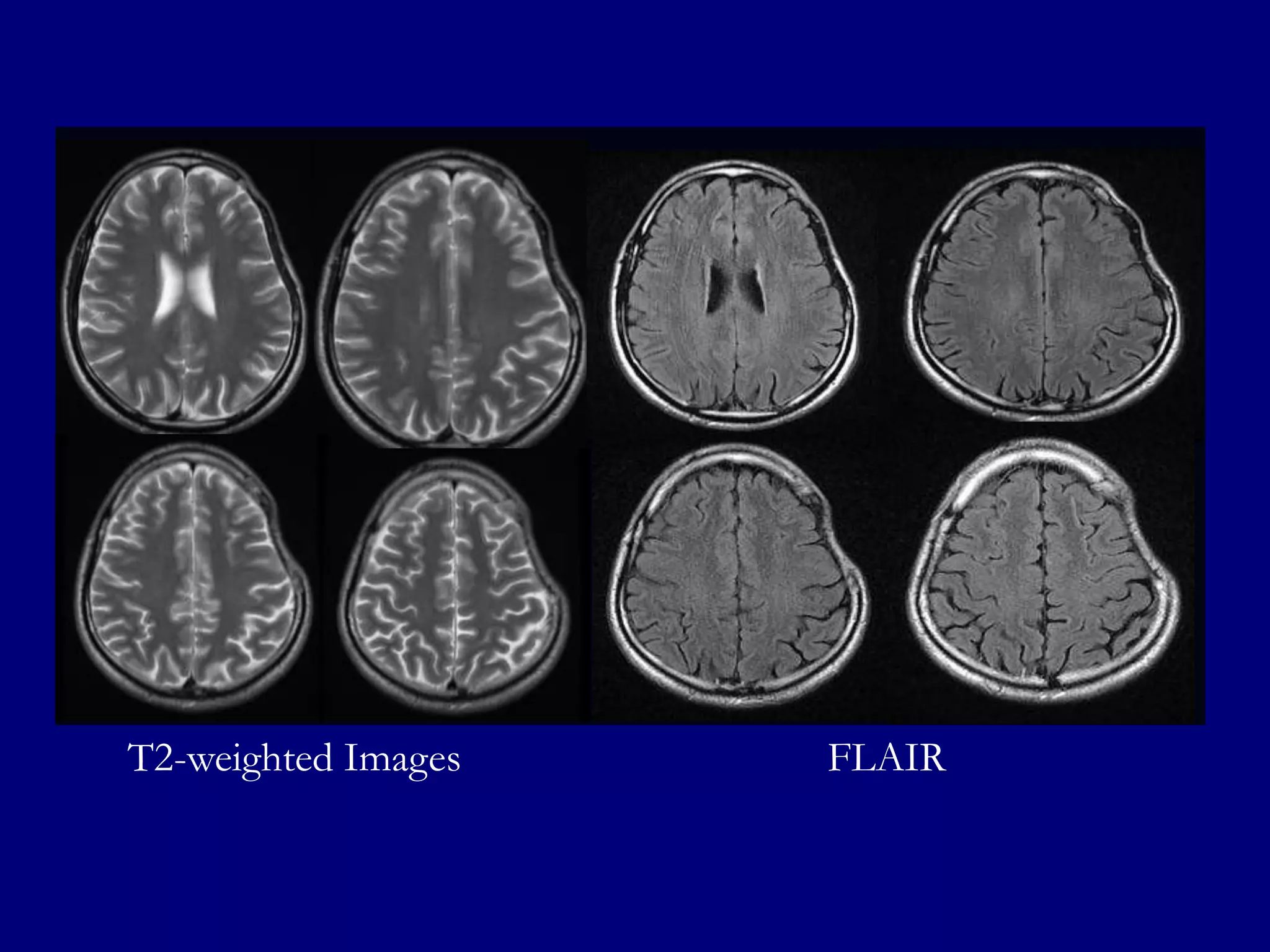
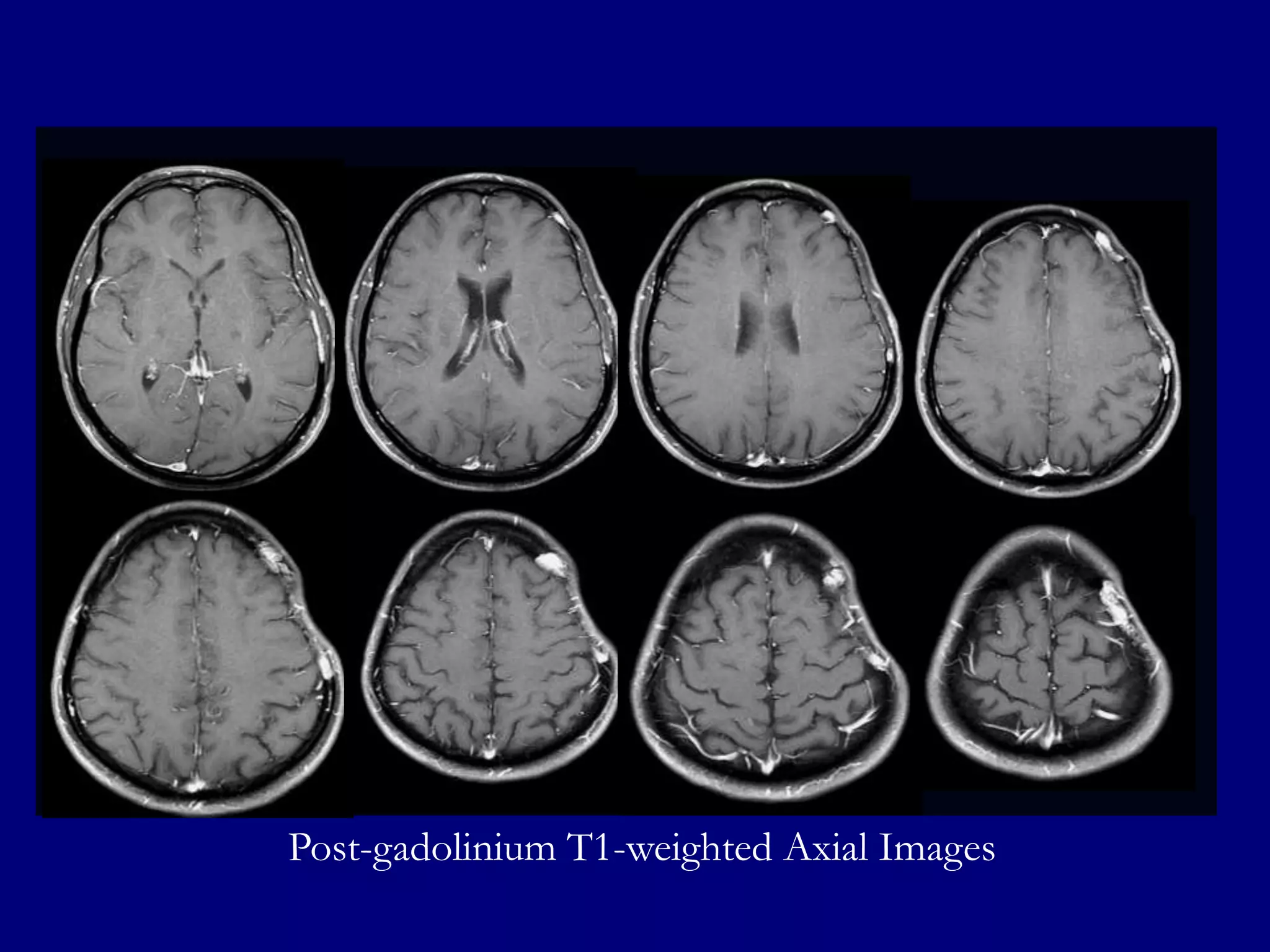
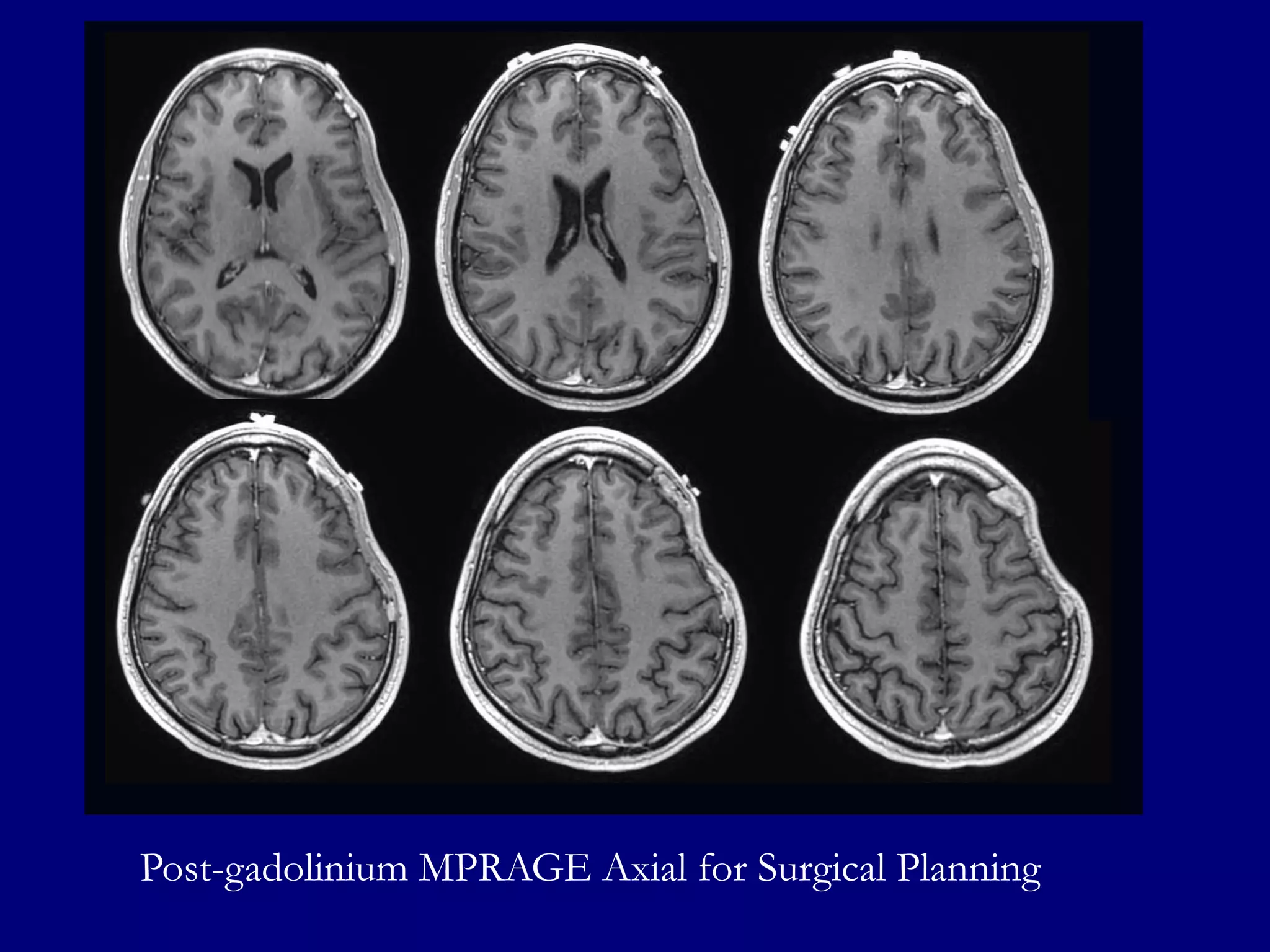
A 37-year-old man presented with right-sided numbness and headaches. Brain imaging showed hyperdense lesions in the left frontal and parietal lobes. MRI revealed well-defined hyperintense lesions on FLAIR and T2-weighted imaging that enhanced homogenously on post-gadolinium images. Spectroscopy showed an elevated choline peak. The findings were most consistent with a diagnosis of primary CNS lymphoma.
























![Wilm's tumour - The most common kidney tumor in children - Dr Vishnu A [VCR],...](https://cdn.slidesharecdn.com/ss_thumbnails/vishnu-wilmstumour-210312145616-thumbnail.jpg?width=640&height=640&fit=bounds)

































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









