Downloaded 380 times
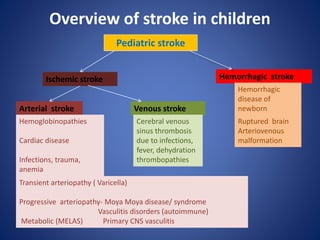

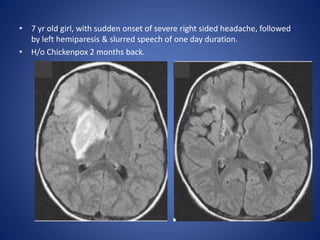
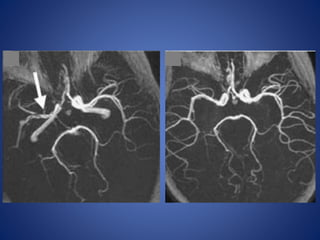
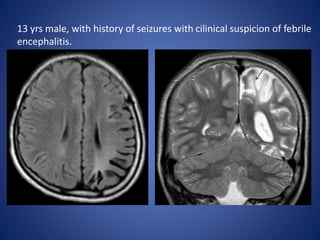
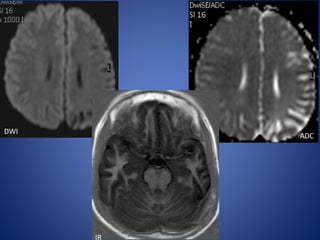
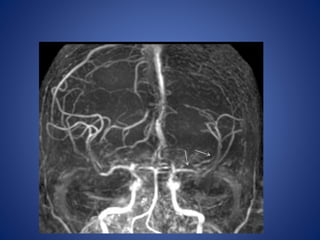
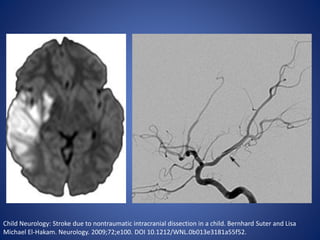


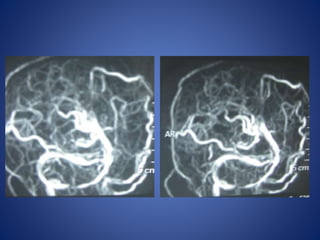
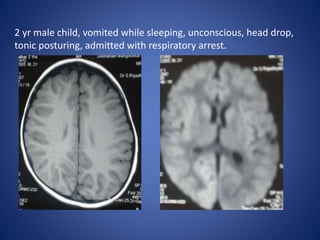
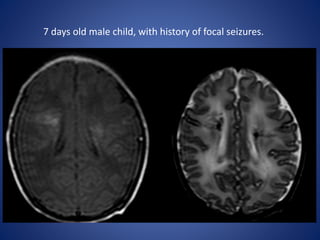
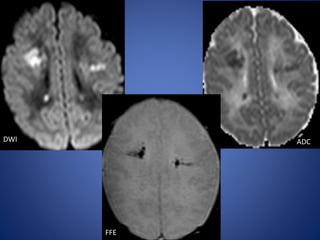
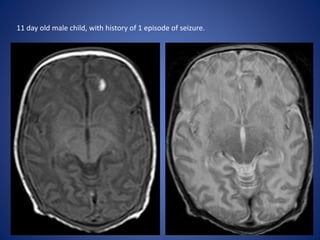
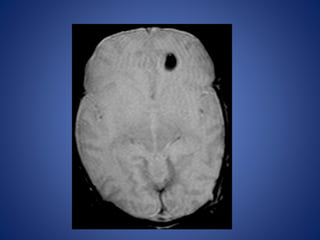
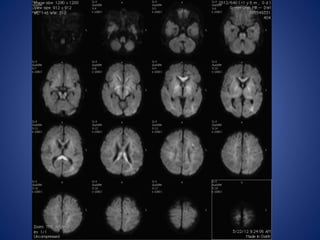
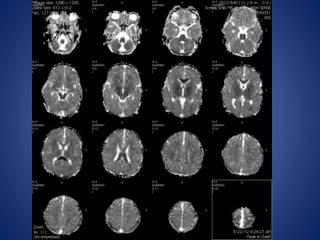
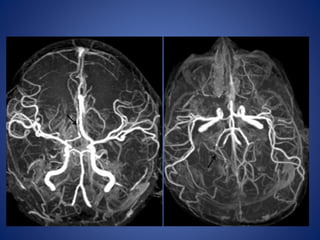


Pediatric stroke can be caused by a variety of factors such as cardiac diseases, infections like varicella, sickle cell disease, moyamoy disease, cerebral sinus thrombosis, and genetic conditions like MELAS. The presentation of pediatric stroke depends on the location and size of the lesion in the brain. Diagnosis involves imaging techniques like CT, MRI, MRA and angiography. Early diagnosis and treatment is important to prevent long term neurological deficits in children.











































































































