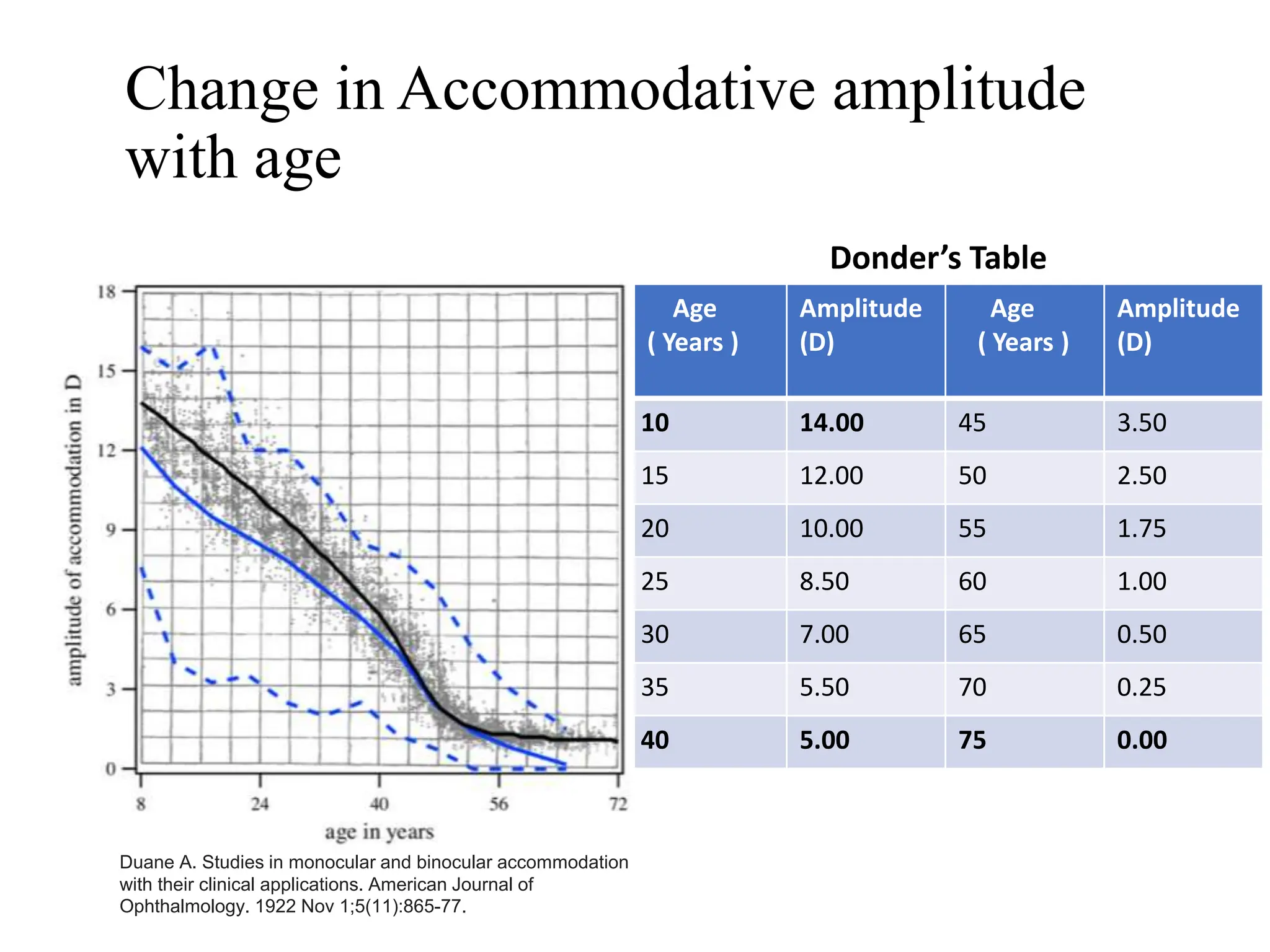
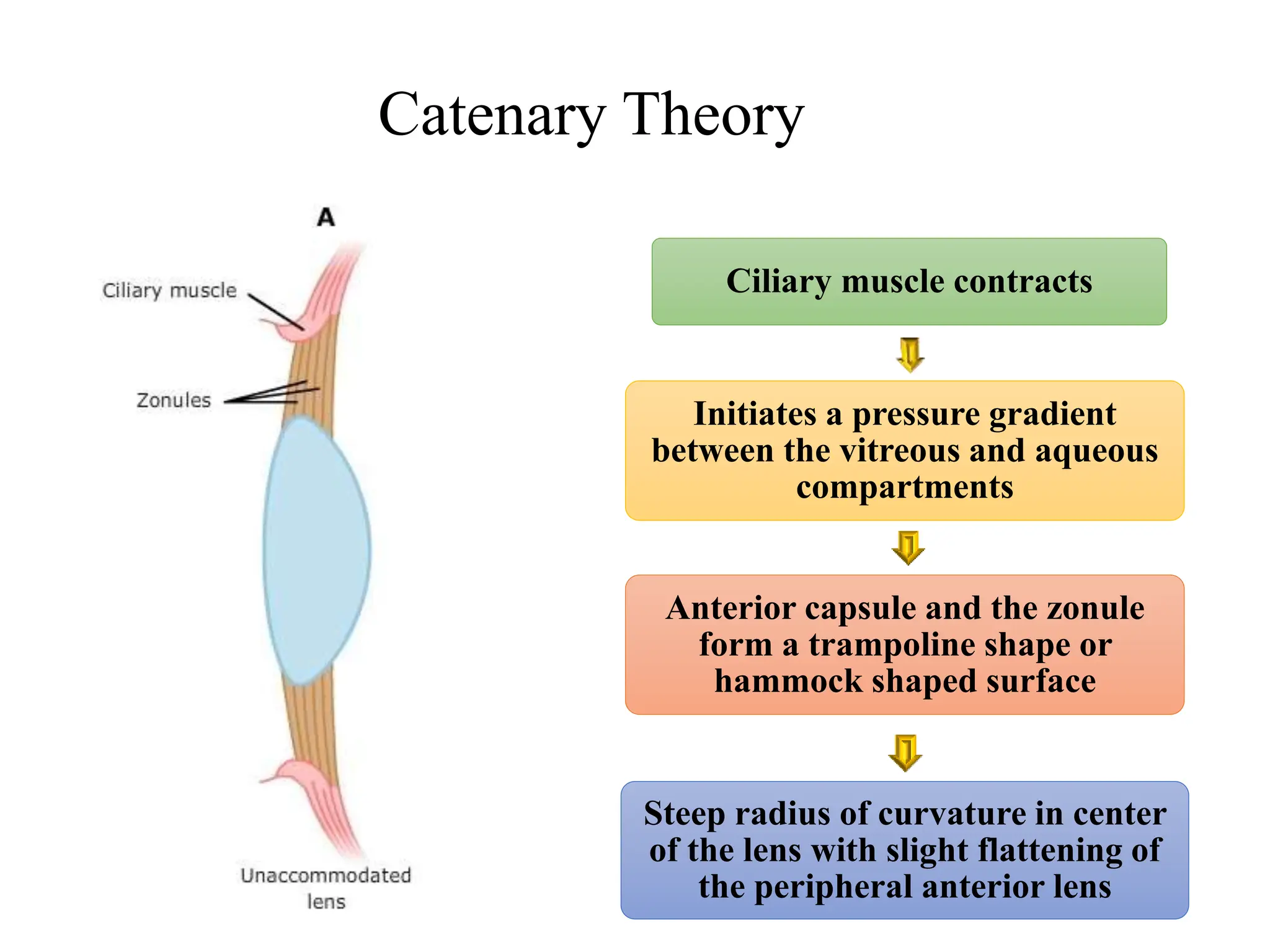
Presbyopia is a normal, age-related loss of the eye's ability to focus on near objects. It is caused by a gradual hardening and loss of elasticity of the lens. Various methods can be used to determine the near prescription addition needed for presbyopia, including taking into account the patient's amplitude of accommodation, age, working distance, and refractive error. Management options include single vision, bifocal, or progressive addition lenses, contact lenses, refractive surgery, and potential future pharmacological treatments.