
Downloaded 37 times

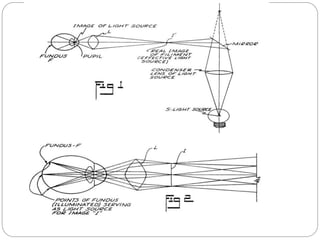
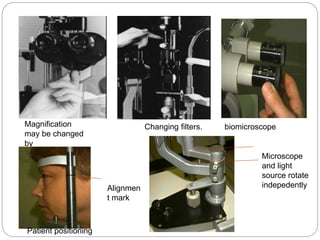

The document discusses slit lamp biomicroscopy, detailing its principles, instrumentation, and various illumination techniques used for examining the anterior segment of the eye. It covers historical milestones in the development of the device, types of slit lamps, and operational components, as well as diagnostic and therapeutic applications in eye care. Additionally, it provides insights into patient positioning and various examinations including the evaluation of the conjunctiva, cornea, and meibomian glands.























































































