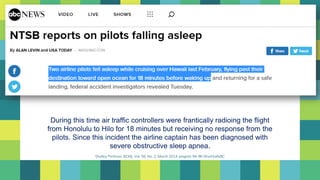
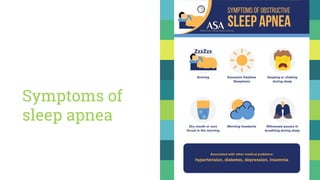
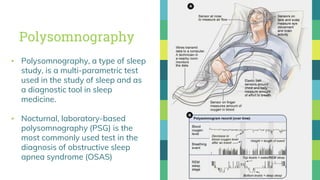
During a flight from Honolulu to Hilo, air traffic controllers were unable to contact the pilots for 18 minutes. Since this incident, the airline captain was diagnosed with severe obstructive sleep apnea. Sleep apnea is a sleep disorder where breathing is interrupted during sleep by pauses or shallow breathing and affects 3.6% of people in North India. The gold standard test for diagnosing sleep apnea is an overnight sleep study called polysomnography. Positive airway pressure therapy using CPAP is very effective at reducing sleep apnea symptoms and improving quality of life.




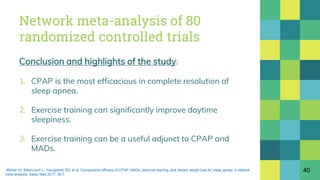
![Network meta-analysis of 80
randomized controlled trials
Objective:
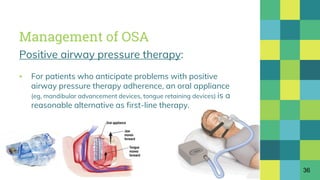
▪ To synthesize evidence from available studies on the
relative efficacies of CPAP, mandibular advancement
device (MAD), supervised aerobic exercise training and
dietary weight loss in patients with OSA.
Results:
▪ CPAP decreased AHI the most [by 25.27 events/hour
(22.03 to 28.52)] followed by exercise training, MADs
and dietary weight loss.
39Iftikhar IH, Bittencourt L, Youngstedt SD, et al. Comparative efficacy of CPAP, MADs, exercise-training, and dietary weight loss for sleep apnea: a network
meta-analysis. Sleep Med 2017; 30:7.](https://image.slidesharecdn.com/sleepapnea-180309072424/85/Sleep-apnea-39-320.jpg)















































![OBSTRUCTIVE SLEEP APNEA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/obstructivesleepapneaautosaved-240801041633-6b724373-thumbnail.jpg?width=640&height=640&fit=bounds)










![Newer drugs in management of copd [2018 update]](https://cdn.slidesharecdn.com/ss_thumbnails/newerdrugsinmanagementofcopd2018update-180309071249-thumbnail.jpg?width=640&height=640&fit=bounds)































