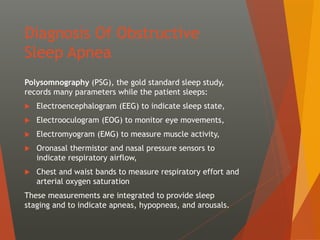
The document provides an overview of the diagnosis and management of obstructive sleep apnea (OSA), particularly emphasizing polysomnography as the gold standard for diagnosis. It discusses treatment options such as positive airway pressure therapy, behavioral therapies, oral devices, surgical interventions, and adjunctive therapies, highlighting CPAP as the mainstay treatment for OSA. Additionally, it covers various types of apneas, sleep study protocols, and the importance of follow-up assessments to evaluate treatment efficacy.







































![ Laser-assisted uvulopalatoplasty- involving removal
of the uvula and a part of the soft palate with a
carbon dioxide laser.
Radiofrequency volumetric tissue reduction (i.e.,
radiofrequency ablation [RFA]), a minimally invasive
technique, has been employed to treat turbinate
hypertrophy and reduce the size of the base of the
tongue.
Genioglossus advancement with hyoid myotomy
involves movement of the tongue forward without
moving the mandible, with the leading aim of
achieving a larger-caliber airway.](https://image.slidesharecdn.com/osa-190916140003/85/Obstructive-Sleep-Apnea-42-320.jpg)























































































