Skin and mucous membrane drugs
•Download as PPTX, PDF•
26 likes•10,920 views

The document discusses various topical agents used in dermatology. It describes emollients like mineral oil and glycerin that soothe skin, protectants like talc and starch that bind to the skin surface, and astringents like acetic acid and tannic acid that precipitate skin proteins. It outlines the differences between creams, lotions, and ointments. It also covers counterirritants, keratolytics, antifungals, phototherapy agents, sunscreens, acne medications, and topical corticosteroids and antipruritics to treat inflammation and itching.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Skin and mucous membrane drugs
Similar to Skin and mucous membrane drugs (20)
More from Raghu Prasada
More from Raghu Prasada (20)
Recently uploaded
Recently uploaded (20)
Skin and mucous membrane drugs
- 1. Dr. RAGHU PRASADA M S MBBS,MD ASSISTANT PROFESSOR DEPT. OF PHARMACOLOGY SSIMS & RC.
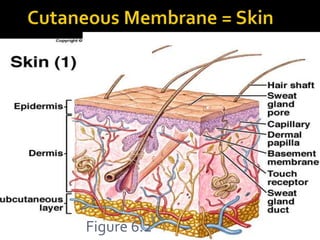
- 2. Figure 6.2
- 3. Are inert substances which sooth inflamed/denuded mucosa or skin by preventing contact with air/ irritants in the surroundings. Liquorice Methylcellulose Propylene glycol Glycerine
- 4. Indication: To soften and soothe rough, dry skin and increase absorbability of topical medications Directions: Apply as necessary or as prescribed; generally after showering/bathing and pat drying; apply liberally to affected areas Olive oil, sesame oil, cocoa butter, liquid paraffin
- 5. They are finely powdered, inert and insoluble solids capable of binding to their surface Magnesium/zinc stearate Talc-hydrous megnesium silicate Calamine Starch Boric acid Aloe vera gel Polyvinyl polymer
- 6. Astringents are agents which precipitate surface protiens and protect the under lying tissue Best used in eczema where vesicular or draining lesions are present Acetic Acid 5% (white vinegar) – especially useful in Pseudomonas infections Burow’s Solution (others) Potassium Permanganate Tannic acid Zinc
- 7. Creams: Less greasy and most acceptable to patient Applies more easily Penetrates skin well Works well in intertriginous and hairy areas Can be drying Have a cooling effect Easy to wash off Lotions: more water content and less viscous than creams Ointments: Petrolatum based Alleviates dryness by prevention of evaporation Removes scales Enables medication to penetrates skin well Water repellant Remains on the skin Occlusive and protective Soothing and lubricating
- 8. They stimulate the sensory nerve endings and induce inflammation at the site of application Rubificiants –irritation+hyperemia+sensory stimulation Vesicants –strong irritation+hyperemia +sensory stimulation+ capillary permeability
- 9. Volatile oils- turpentine oil, Clove oil, eucalyptus oil, camphor, menthol Mustard seeds, capsicum, canthridin Methyl salicylate Alcohol
- 10. Corrosive Podophyllium resin Silver nitrate Phenol Tri chloro acetic acid
- 11. These are the substances that dissolve the intercellular cementing substance and cause peeling of the superficial layers of skin Treatment -Warts, cones, calluses, severe xerosis Salicylic acid, lactic acid, urea, sulfur Resorcinol –antiseptic, antifungal, local irritant Urea –hygroscopic, with steroid Benzyl peroxide- keratolytic effects of acne
- 12. Selenium sulfide Zinc pyrithione Corticosteroids Immidazole antifungals Sulfur, coal tar
- 13. Increase sensitivity to solar radiation Psoralen Methoxsalen Trioxsalen
- 14. Calcipotriol- supresses epidermal proliferation Tazarotene –synthetic retinoid Coaltar –exerts phototoxic action Photochemotherapy-PUVA Acitretin-synthetic retinoid Etanercept Methotrexate
- 15. Tegrin cream and lotion Medotar ointment PsoriGel gel Polytar and Tegrin soaps Tegrin, T/Gel, and other shampoos Indication: to relieve and control itching, and flaking skin associated with psoriasis and seborrhea as well as eczema Directions: Depending on product 1-4 times daily
- 16. Contraindications: Hypersensitivity Precautions: Do not use on broken skin, genital or rectal area except on the advise of your health care provider. Photosensitivity x 24hr after application May stain light colored hair Warning: High concentrations of some chemicals in coal tar may cause cancer. Concentrations of 0.5% to 5% appear to be safe.
- 17. Hydroquinone Monobenzene Azelaic acid
- 18. These are the agents that protect the skin from the effects of UV rays photo-aging and photo-toxicity UVB screens –PABA, benzophenones Cinnamates, Salicylates UVA screens- Avobenzene, Oxybenzene, Titanium dioxide, Zinc oxide Reflection of UV rays-Physical – petroleum jelly, zinc oxide, calamine
- 19. Topical therapy-benzoyl peroxide benzoic acid antibacterial, comedolytic, keratolytic action Retinoic acid –topically reduces hyperkeratinization, comedolytic and decreases pigmentation and prevents formation of comedones Adapalene – synthetic tretinoin Isotretinoin-orally Topical antibiotics Azelaic acid-from pityrosporium ovale inhibits aerobic and anaerobic organisms. Also used for melasma Systemic therapy
- 21. Antiinflammatory topicals Hydrocortisone creams, 0.5% to 1% Antipruritics and others 1. Benadryl (diphenhydramine 25-50mg q6h prn) 2. Calamine Lotion (zinc oxide and ferric oxide used as a mild astringent) 3. Caladryl Lotion (both of above) 4. Burrow’s solution