Downloaded 1,027 times
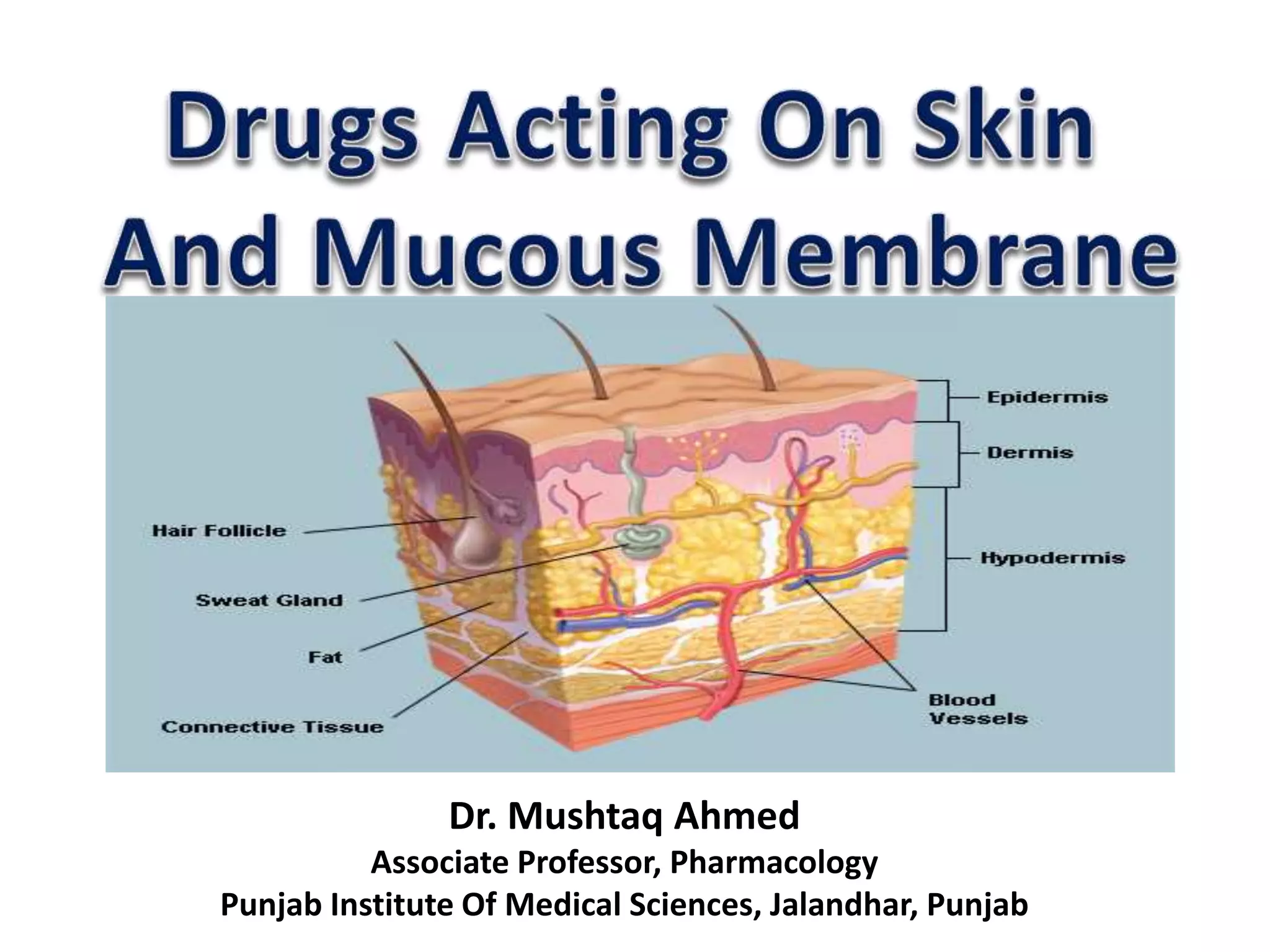
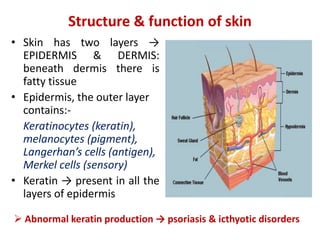


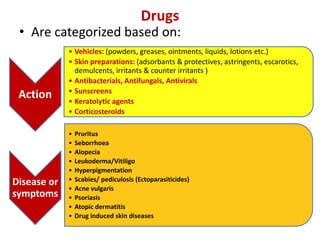







This document provides information on the structure and function of skin, treatment of various skin disorders, and drugs used for different skin conditions. It discusses: - The structure of the epidermis and dermis layers of skin and their functions. - Topical, systemic, and other modes of treating skin disorders. - Factors affecting absorption of topical drugs and examples of transdermal patches. - Classes of drugs categorized by action, vehicles, and skin preparations. - Specific drugs and classes used to treat conditions like pruritus, seborrhea, alopecia, pigment disorders, ectoparasitic infections, acne, and others.



































































