Download to read offline
![Sikkim Manipal University
Assignment BLOO43
Roll No-621132459(Vipin Pant)4rh semester
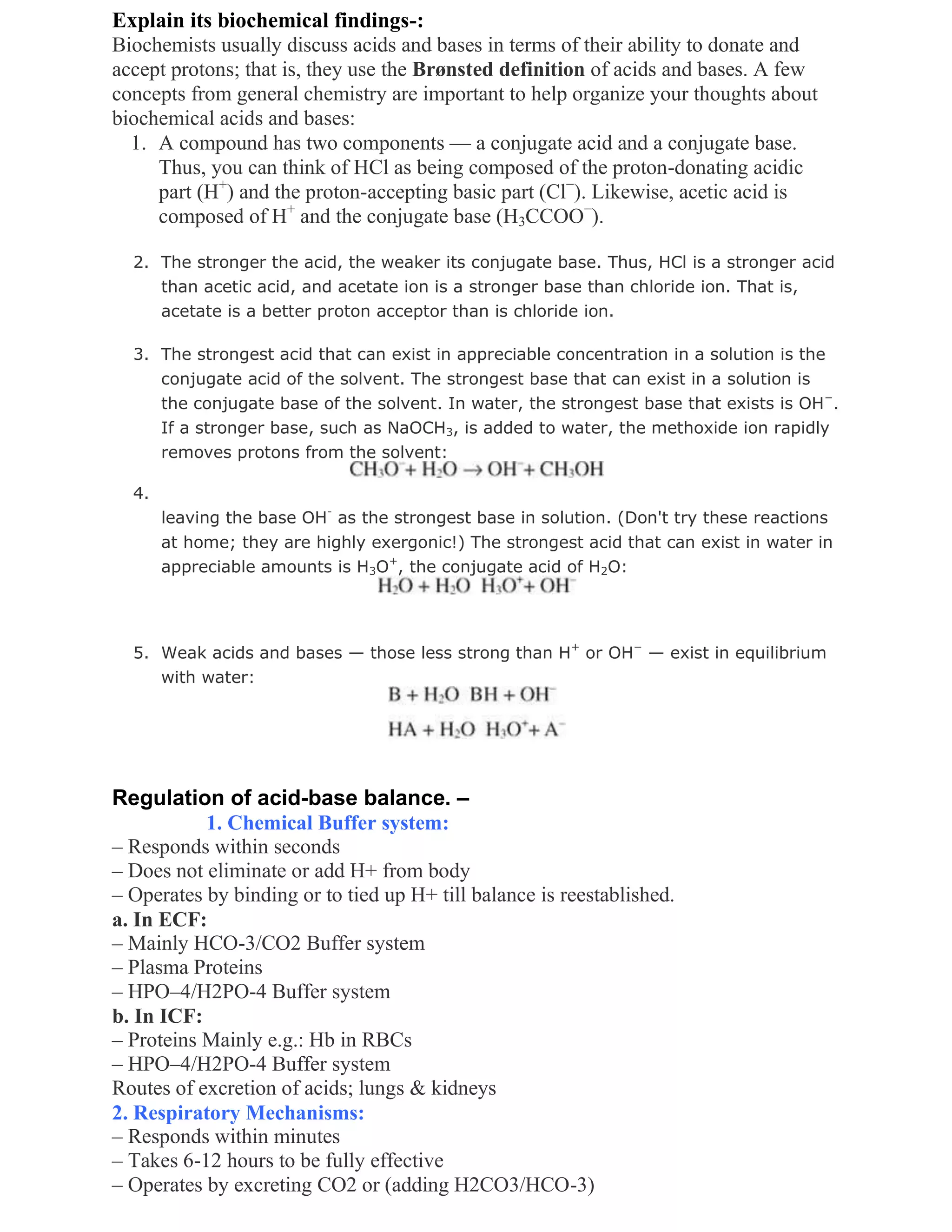
1) What are acid-base disorders? Explain its biochemical findings. Add a
note on regulation of acid-base balance
Ans- Acid–base imbalance is an abnormality of the human body's normal balance of
acids and bases that causes the plasma pH to deviate out of the normal range (7.35 to
7.45). In the fetus, the normal range differs based on which umbilical vessel is
sampled (umbilical vein pH is normally 7.25 to 7.45; umbilical artery pH is normally
7.18 to 7.38).[1] It can exist in varying levels of severity, some life-threatening.
Classification
A Davenport diagram illustrates acid–base imbalance graphically.
An excess of acid is called acidosis and an excess in bases is called alkalosis. The
process that causes the imbalance is classified based on theetiology of the disturbance
(respiratory or metabolic) and the direction of change in pH (acidosis or alkalosis).
This yields the following four basic processes:
process pH carbon dioxide compensation
metabolic acidosis down down respiratory
respiratory acidosis down up renal
metabolic alkalosis up up respiratory
respiratory alkalosis up down renal
]Mixed disorders
The presence of only one of the above derangements is called a simple acid–base
disorder. In a mixed disorder more than one is occurring at the same time.[2] Mixed
disorders may feature an acidosis and alkosis at the same time that partially counteract
each other, or there can be two different conditions affecting the pH in the same
direction. The phrase "mixed acidosis", for example, refers to metabolic acidosis in
conjunction withrespiratory acidosis. Any combination is possible, except concurrent
respiratory acidosis and respiratory alkalosis, since a person cannot breathe too fast
and too slow at the same time.](https://image.slidesharecdn.com/sikkimmanipaluniversity-secoun-130306214119-phpapp01/75/Sikkim-manipal-university-secoun-1-2048.jpg)
![3. Renal Mechanisms:
• Responds slowly (effectively in 3-5 days)
• Eliminates excess Acids or Base from body
• The most powerful mechanism
e.g. i. HCO-3/CO2 Buffer system
ii. NH3/NH+4 Buffer system
iii. HPO–4/H2PO-4 Buffer system
Chemical Buffer System
• Consists of a ‗pair of substances‘ present in a mixture of a solution that ‗minimizes
pH changes‘ when an ‗acid or base‘ is ‗added or removed‘ from the solution.
• Consists of;
1. Carbonic Acid – Bicarbonate Buffer System
2. Phosphate Buffer system
3. Protein Buffer system
Chemical Buffer System of ECF
1. Bicarbonate Buffer System: H2CO3/NaHCO3
consists of H2CO3 (weak Acid) + NaHCO3 (Bicarbonate salt)
– CO2 + H2O ↔H2CO3 ↔ H+ + HCO-3
– NaHCO3 ↔ Na+ + HCO-3 → H2CO3 → CO2 + H2O
Bicarbonate buffer system is quantitatively the most powerful ECF buffer system
Its two components HCO-3 & CO2 are precisely regulated by kidneys & lungs.
2. Phosphate Buffer System:
– Not of major importance in ECF
– Only 8% of the conc. of HCO-3 Buffer system
– Comprised of HPO–4/H2PO-4
– Plays major role in ICF & in Renal tubules
3. Proteins: (ICF proteins, Hb, Plasma proteins)
– Excellent buffers as proteins contain both Acidic & Basic groups.
– More important in ICF H2CO3 ← H2O + CO2
HCO-3 + H+ + HbO2 ↔ H.Hb + O2
– In RBCs, Hb is important
– 60-70% of total chemical buffering of body fluids inside the
cells & in ICF is by proteins.
– Hb buffers H+ ions generated by H2CO3
– Proteins are the most abundant buffers in cells & in blood
– Histidine and Cysteine are the two A. Acids that contribute
most of the buffering capacity of proteins
Respiratory Mechanisms in Regulation of Acid-Base
• Second line of defense against acid base disturbances
• Operates through regulation of ECF CO2 concentration by lungs
• Effectiveness between 50-75% [feedback gain is 1-3 i.e. fall in pH
from 7.4 to 7.0 is returned by Resp System to 7.2 to 7.3 within 3-12
minutes]
2) Discuss the advantages of automation in clinical biochemistry
laboratory. Make a list of few (at least five) automated instruments
available for biochemical analysis. Discuss the principle of each .](https://image.slidesharecdn.com/sikkimmanipaluniversity-secoun-130306214119-phpapp01/75/Sikkim-manipal-university-secoun-3-2048.jpg)



The document discusses acid-base disorders and summarizes: 1) Acid-base disorders occur when the body's normal balance of acids and bases deviates from the normal pH range, causing acidosis or alkalosis. Disorders can be classified as respiratory or metabolic based on their etiology. 2) Biochemical findings include concepts of acids and bases donating and accepting protons. The strongest acid and base present in water are H3O+ and OH-. 3) Regulation of acid-base balance involves chemical buffer systems, respiratory mechanisms, and renal mechanisms working together to precisely control pH levels.




















































































