This document discusses acid-base balance in the human body. It explains that pH is tightly regulated through carbon dioxide tension, plasma bicarbonate levels, and renal mechanisms. The lungs, kidneys, and cells all work to maintain homeostasis. When acid-base balance is disturbed, the condition can be either respiratory or metabolic in nature. The document outlines the various buffer systems, including bicarbonate, phosphate and proteins. It also explains how the lungs and kidneys work to compensate for respiratory and metabolic acid-base disturbances respectively.

![Human Acid-base Homeostasis
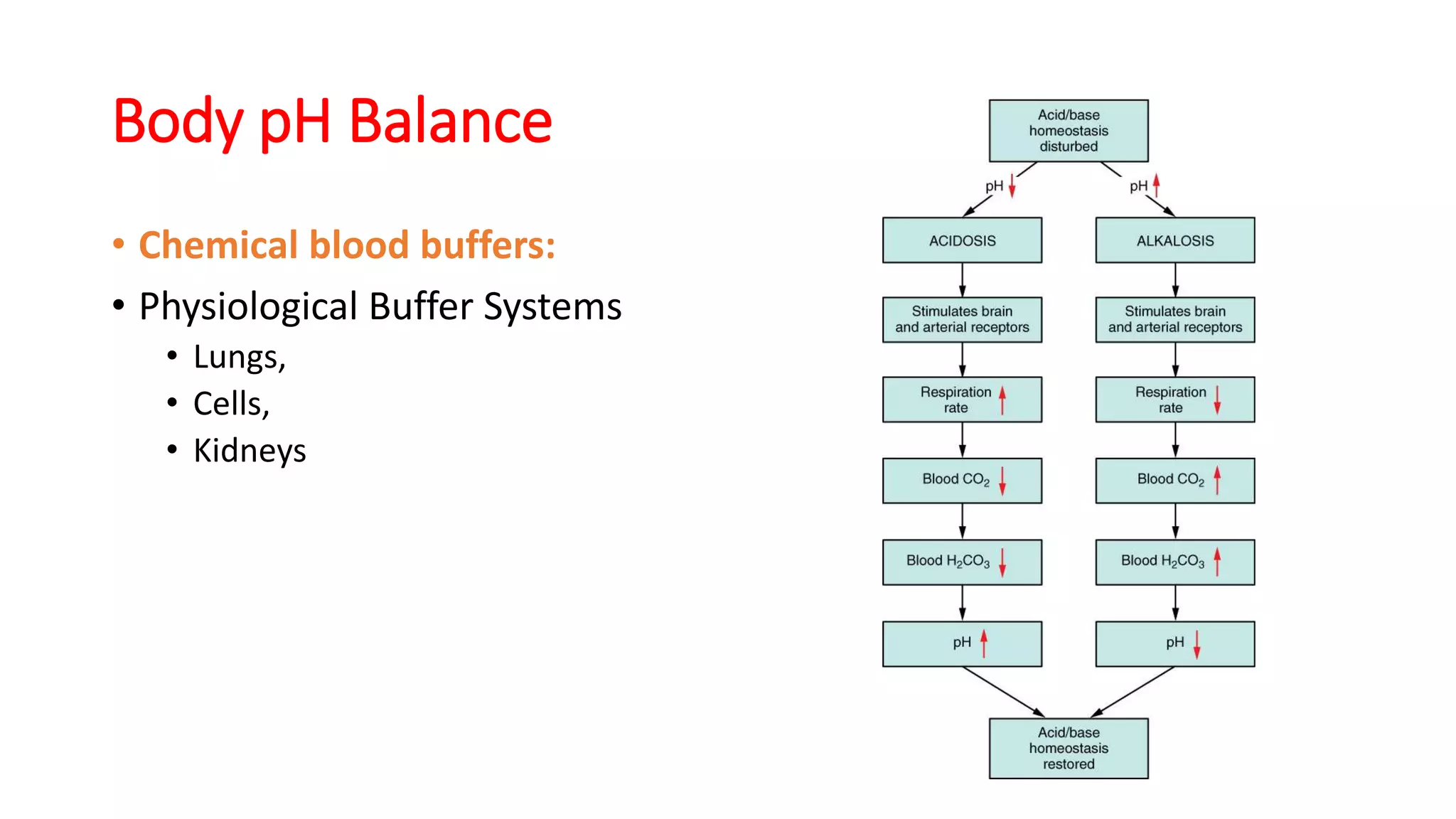
• Tight regulation:
• CO2 tension
• by respiratory excretion (of volatile acids)
• Plasma bicarbonate [HCO3
-]
• By renal HCO3
- reabsorption and
• Elimination of protons produced by metabolism
• pH is determined by CO2 tension and [HCO3
-]](https://image.slidesharecdn.com/acidbasebalancekabsom-200305112811/75/Acid-base-balance-in-surgery-2-2048.jpg)


![Normal Values
• [HCO3
-] ~ 24 mM
• PaCO2 = 38 torr
• pH ~ 7.42
• Plasma HCO3
- regulation by
• reclaiming filtered HCO3
- and
• generating new HCO3
- (carboanhydrase)
• ( to replace the lost internally titrating metabolic acid and
externally from the GI tract)
• Production of 1 mmol of acid/kg body weight per
day (60 kg=60 mmol/day)](https://image.slidesharecdn.com/acidbasebalancekabsom-200305112811/75/Acid-base-balance-in-surgery-7-2048.jpg)