Downloaded 44 times


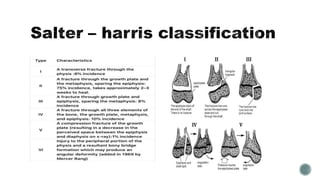
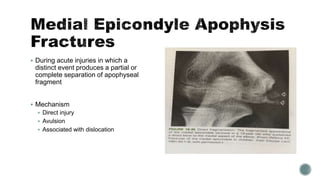
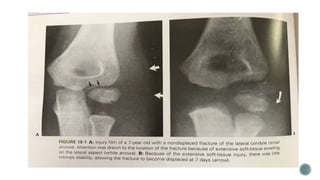


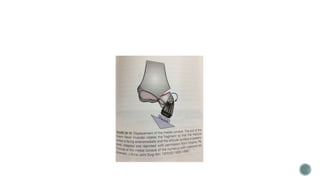



This document discusses various types of elbow fractures that can occur in children, including medial epicondyle apophysis fractures, pulled elbow syndrome, lateral condylar fractures, capitellar fractures, and medial condylar fractures. It provides details on the mechanisms of injury, classification systems, stages of displacement, and treatment approaches for each type of fracture. Key facts covered include that lateral condylar fractures can cross the physis or extend into the trochlear cartilage, and medial condylar fractures have both an intra-articular and extra-articular component. Classification systems such as those proposed by Milch and Weiss are described.























































































