Downloaded 222 times
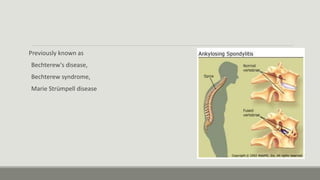
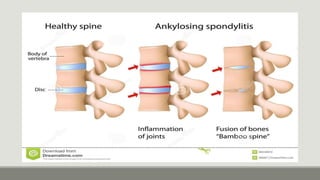
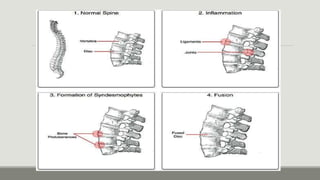
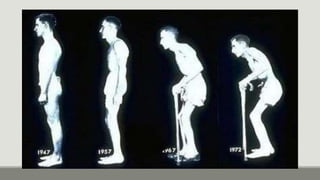



Ankylosing spondylitis is a form of arthritis that primarily affects the spine and sacroiliac joints, causing fusion of the spine over time. It typically develops in young adults aged 18-30 and is more common in men. Genetics play a role, as 90% of patients have the HLA-B27 gene. Symptoms include chronic lower back pain and stiffness that worsens with inactivity. Diagnosis involves blood tests, x-rays showing spinal changes, and assessment of limited range of motion. Treatment focuses on reducing inflammation and pain through NSAIDs, DMARDs, biologics that target tumor necrosis factor-alpha, and occasionally surgery for deformities.























































































