Downloaded 43 times







![ Another prospective, surgeon randomized trial conducted by Gaston et al. also
revealed that there was no statistical difference in radiographic outcomes of
lateral vs. cross pinning of type III fractures [14].
Mahan et al. analyzed surgeon preference of cross pins vs. lateral only pinning
after the prospective randomized control trial conducted by Kocher in 2007.
Consistent with our result, Mahan et al. found that there was a statistically
significant change in surgeon preference from cross pinning before the trial to
lateral only pinning after the trial](https://image.slidesharecdn.com/pediatricsupracondylarhumerusfractures-180622024526/85/Pediatric-supracondylar-humerus-fractures-46-320.jpg)
![References
[1] Houshian, S., Mehdi, B. and Larsen, M.S. (2001) The Epidemiology of Elbow Fracture in Children: Analysis of 355 Fractures, with Special
Reference to Supracondylar Humerus Fractures. Journal of Orthopaedic Science, 6, 312-315. http://dx.doi.org/10.1007/s007760100024
[2] Mahan, S.T., May, C.D. and Kocher, M.S. (2007) Operative Management of Displaced Flexion Supracondylar Fractures in Children. Journal
of Pediatric Orthopaedics, 27, 551-556. http://dx.doi.org/10.1097/01.bpb.0000279032.04892.6c
[3] Lee, Y.H., et al. (2008) Three Lateral Divergent or Parallel Pin Fixations for the Treatment of Displaced Supracondylar Humerus Fractures
in Children. Journal of Pediatric Orthopaedics, 28, 417-422. http://dx.doi.org/10.1097/BPO.0b013e318173e13d
[4] Kim, W.Y., Chandru, R., Bonshahi, A., et al. (2003) Displaced Supracondylar Humeral Fractures in Children: Results of a National Survey of
Pediatric Orthopedic Consultants. Injury, 34, 274-277. http://dx.doi.org/10.1016/S0020-1383(02)00321-2
[5] Lee, S.S., Mahar, A.T., Miesen, D., et al. (2002) Displaced Pediatric Supracondylar Humerus Fractures: Biomechanical Analysis of
Percutaneous Pinning Techniques. Journal of Pediatric Orthopaedics, 22, 440-443. http://dx.doi.org/10.1097/01241398-200207000-00005
[6] Kocher, M.S., Kasser, J.R., Waters, P.M., et al. (2007) Lateral Entry Compared with Medial and Lateral Entry Pin Fixation for Completely
Displaced Supracondylar Humeral Fractures in Children. A Randomized Control Trial. The Journal of Bone & Joint Surgery, 89, 706-712.
http://dx.doi.org/10.2106/JBJS.F.00379
[7] Brauer, C.A., Lee, B.M., Bae, D.S., et al. (2007) A Systematic Review of Medial and Lateral Entry Pinning Versus Lateral Entry Pinning for
Supracondylar Fractures of the Humerus. Journal of Pediatric Orthopaedics, 27, 181-186. http://dx.doi.org/10.1097/bpo.0b013e3180316cf1](https://image.slidesharecdn.com/pediatricsupracondylarhumerusfractures-180622024526/85/Pediatric-supracondylar-humerus-fractures-50-320.jpg)
![8] Brown, I.C. and Zinar, D.M. (1995) Traumatic and Iatrogenic Neurological Complications after Supracondylar Humerus Fractures in Children. Journal of
Pediatric Orthopaedics, 14, 440-443. http://dx.doi.org/10.1097/01241398-199507000-00005
[9] Bronwyn, S.L., Jackman, H., Tennant, S., et al. (2010) Iatrogenic Ulnar Nerve Injury after the Surgical Treatment of Displaced Supracondylar Fractures of
the Humerus: Number Needed to Harm, A Systematic Review. Journal of Pediatric Orthopaedics, 30, 430-436.
http://dx.doi.org/10.1097/BPO.0b013e3181e00c0d
[10] Zionts, L.E., McKellop, H.A. and Hathaway, R. (1994) Torsional Strength of Pin Configurations Used to Fix Supracondylar Fractures of the Humerus in
Children. The Journal of Bone & Joint Surgery, 76, 253-256.
[11] Zamzam, M.M. and Bakarman, K.A. (2009) Treatment of Displaced Supracondylar Humerus Fractures among Children: Crossed versus Lateral Pinning.
Injury, 40, 625-630. http://dx.doi.org/10.1016/j.injury.2008.10.029
[12] Larson, L., Firoozbakhsh, K., Passarelli, R. and Bosch, P. (2006) Biomechanical Analysis of Pinning Techniques for Pediatric Supracondylar Humerus
Fractures. Journal of Pediatric Orthopaedics, 26, 573-578. http://dx.doi.org/10.1097/01.bpo.0000230336.26652.1c
[13] Tripuraneni, K.R., Bosch, P.P., Schwend, R.M. and Yaste, J.J. (2009) Prospective, Surgeon-Randomized Evaluation of Crossed Pins versus Lateral Pins for
Unstable Supracondylar Humerus Fractures in Children. Journal of Pediatric Orthopaedics Part B, 18, 93-98.
[14] Gaston, R.G., Cates, T.B., Devito, D., et al. (2010) Medial and Lateral Pin Versus Lateral-Entry Pin Fixation for Type 3 Supracondylar Fractures in
Children: A Prospective, Surgeon-Randomized Study. Journal of Pediatric Orthopaedics, 30, 799-806. http://dx.doi.org/10.1097/BPO.0b013e3181f73d59
[15] Mahan, S.T., Osborn, E., Bae, D.S., et al. (2012) Changing Practice Patterns: The Impact of a RandomizedClinical Trial on Surgeons Preference for
Treatmentof Type 3 Supracondylar Humerus Fractures. Journal of Pediatric Orthopaedics, 32, 340-345. http://dx.doi.org/10.1097/BPO.0b013e3182519d1d](https://image.slidesharecdn.com/pediatricsupracondylarhumerusfractures-180622024526/85/Pediatric-supracondylar-humerus-fractures-51-320.jpg)

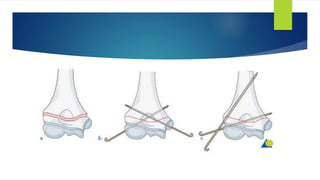
This document summarizes a study on operative management of pediatric supracondylar humerus fractures. The study found that between 2006-2008, medial pins were routinely used for type III fractures, but between 2009-2011 there was an effort to minimize medial pin use. For type III fractures, there was a statistically significant decrease in the use of cross pin fixation between the two time periods. Clinical outcomes such as nerve injury, malalignment, and re-operation rates were comparable between the groups that received lateral-only pinning versus cross pinning. The study concludes that lateral-only pinning can effectively treat these fractures while avoiding risks of iatrogenic nerve injury associated with medial pinning.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














