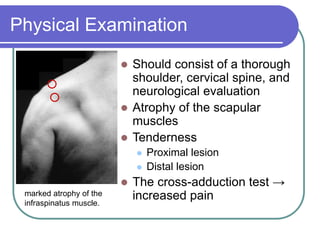
The suprascapular nerve can become entrapped at the suprascapular notch or spinoglenoid notch, causing shoulder pain and weakness. Entrapment is often due to repetitive microtrauma from overhead activities. Diagnosis involves physical exam finding atrophy and tenderness, as well as electrodiagnostic studies and imaging like MRI. Nonoperative treatments include rest and physical therapy. Surgical treatment involves release of structures compressing the nerve, such as the superior transverse scapular ligament or spinoglenoid ligament. Ganglion cysts can also compress the nerve and may require aspiration.












































![Tip & tricks [Autosaved] - Copy.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/tiptricksautosaved-copy-220902124657-5a096dbd-thumbnail.jpg?width=640&height=640&fit=bounds)



































