
Downloaded 219 times











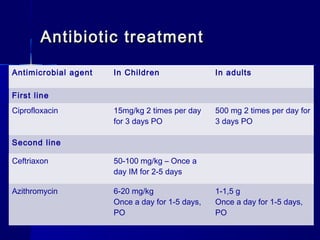
Shigellosis is an intestinal infection caused by Shigella bacteria, leading to severe abdominal cramps, bloody diarrhea, and potential fever. The disease primarily affects young children and is transmitted through fecal-oral routes, often in situations with poor sanitation. Treatment involves antibiotics, rehydration, and management of complications, with isolation of the pathogen from fecal material being the diagnostic gold standard.











































































































