Introduction
• Shigella isnamed after the scientist Shiga who 1st of all isolated the
organism in 1896 from epidemic dysentery in Japan.
• At that time, the organism was called as Shigella shiga.
• But now in Bergey's manual, it is called an Shigella dysenteriae.
• Later on, other species of Shigella were isolated.
• Flexner isolated Shigella flexneri in 1898 in Philippines.
• In 1915, Shigella sonnei was isolated by Sonnei in Denmark.
3.
Morphology
• Gm –vebacilli, short rods
• non-motile (no H antigen), fimbriate,
• non-encapsulated,
• non-spore former,
• It measures 1-3 μm x 0.5 μm in general.
4.
Cultural characteristics
• Theyare aerobes and facultative anaerobes, grow best at 37°, pH 7.4
on ordinary media (pH 6.4 to 7.8 and at 100C to 400C)
• On NA, colonies are small about 2 mm in diameter, circular, convex,
colorless, moderately translucent, smooth surface and entire edges.
• On MA, the colonies are pale or colorless (non lactose fermenter)
except Shigella sonnei which is a late lactose fermenter.
• DCA and SS agar medium are useful selective media, but their growth
is inhibited on Wilson and Blair medium.
• On XLD, Shigella produce pink colonies without black centers.
5.
Biochemical reactions:
• aerobesand facultative anaerobes
• Catalase : positive
• Oxidase : negative
• Urease : negative
• Ferment glucose
• Non-lactose fermenting
• Bile salts resistant: trait useful for selective media
• Reduce nitrates (NO3 to NO2 or N2)
6.
Antigenic structure
• Allthe Shigella possess O antigen and some may possess K antigen
• Those strains that contain K antigen appear as smooth colonies when
grown in agar media.
• K antigen is not useful in serological typing, but can interfere with O
antigen determination.
7.
Taxonomy
• Shigella aredivided into 4 major groups or species which are designed
as A, B, C and D.
• Each group or species is sub-divided into types based on difference
in O antigen. These sub-groups are designated as 1, 2, 3………
• Group A : Shigella dysenteriae 12 serotypes
• Group B : Shigella flexneri
• Group C : Shigella boydii
• Group D : Shigella sonnei
6 serotypes
18 serotypes
1 serotype 17 Colicin types
8.
• Group A:Shigella dysenteriae most serious form of bacillary
dysentery
• Group B : Shigella flexneri shigellosis in underdeveloped
countries
• Group C : Shigella boydii shigellosis in developed countries
• Group D : Shigella sonnei
• On the basis of Mannitol fermentation:
1. Non-mannitol-fermenter: Sh. dysenteria
2. Mannitol-fermenter: Sh. flexneri, Sh. boydii, Sh. sonnei
11.
Pathogenic Determinants ofShigella
1. O antigen: The ability to survive the passage through the host
defenses may be due to O antigen.
2. Invasiveness:
• Virulent Shigella penetrate the mucosa and epithelial cells of the
colon in an uneven manner.
• Intracellular multiplication leads to invasion of adjacent cells,
inflammation and cell death.
3. Other toxins:
• It has a protein toxin (exotoxin or Shiga toxin) which may be
neurotoxic, cytotoxic, and enterotoxic.
• The enterotoxic property is responsible for watery diarrhea.
12.
Characteristics of ShigaToxin
• Enterotoxic, neurotoxic and cytotoxic
• Encoded by chromosomal genes.
• Two domain (A-5B) structure
• Similar to the Shiga-like toxin of
Enterohemorrhagic E. coli (EHEC).
13.
Enterotoxic Effect:
• Adheresto small intestine receptors.
• Blocks absorption (uptake) of electrolytes, glucose, and amino acids
from the intestinal lumen
[Note: This contrasts with the effects of cholera toxin (V. cholerae) and labile toxin
(LT) of Enterotoxigenic E. coli (ETEC) which act by blocking absorption of Na+, but
-
also cause hypersecretion of water and ions of Cl-, K+ (hypokalemia), and HCO3
(loss of bicarbonate buffering capacity leads to metabolic acidosis) out of the
intestine and into the lumen]
Neurotoxic Effect:
• Fever and abdominal cramping are considered signs of neurotoxicity.
14.
Cytotoxic Effect:
• Bsubunit of Shiga toxin binds host cell glycolipid in large intestine.
• A domain is internalized via receptor-mediated endocytosis (coated
pits).
• Causes irreversible inactivation of the 60S ribosomal subunit, thereby
causing:
• Inhibition of protein synthesis,
• Causing cell death,
• Microvasculature damage to the intestine,
• Hemorrhage (blood & fecal leukocytes in stool)
15.
Epidemiology
• Shigellosis isa major cause of diarrheal disease (developing nations).
• Major cause of bacillary dysentery (severe 2nd stage form of shigellosis)
• Leading cause of infant diarrhea and mortality in developing countries.
• The highest incidence of Shigellosis occur in areas of poor sanitation
and where water supplies are polluted.
• Basically, the S. dysentery causes most severe form of dysentery.
• The infection due to S. flexneri and S. boydii are less severe
and common in tropical and sub-tropical countries.
• S. sonnei is mostly shown in children.
• Low infectious dose (102-104 CFU) with 1-3 day incubation
period.
16.
Habitat and Transmission
•Shigella species are found only in the human intestinal tract.
• Carriers of pathogenic strains can excrete the organism up to two
weeks after infection and occasionally for longer periods.
• Shigella are killed by drying.
• Shigella are transmitted by the fecal-oral rout.
• Other modes of transmission include ingestion of contaminated food
or water, contact with infected objects, or sexual contact.
• Spread is always from a human resource and generally involves
one of the five fs: food, fingers,feces, flies or fomites.
• This is in contrast to salmonellae, which are often spread to humans
from infected animals.
17.
Clinical Syndromes (Shigellosis)
•Ranges from asymptomatic infection to sever bacillary dysentery.
• Process involves:
1. Ingestion
2. Non-invasive colonization and cell multiplication
3. Production of the enterotoxin by the pathogenic bacteria in the
small intestine.
• Two-stage disease: watery diarrhea changing to dysentery with
frequent small stools with blood and mucus, tenesmus, cramps, fever.
18.
Early stage:
• Waterydiarrhea attributed to the enterotoxic activity of Shiga toxin.
• Fever attributed to neurotoxic activity of toxin.
Second stage:
• Adherence to and tissue invasion of large intestine.
• Typical symptoms of dysentery.
• Cytotoxic activity of Shiga toxin increases severity.
19.
Pathogenesi
s
• Shigella dysentery,form a powerful exotoxin, it is associated with
epidemics of bacillary dysentery.
• In man, shigellosis begins with symptoms of acute gastro-enteritis
which is accompanied by abdominal pain and diarrhea.
• As it progresses, diarrhea becomes more frequent and is usually
accompanied colicky pain.
• Later diarrhea losses its fecal characteristic and is followed by mucus
with pus and blood.
• The disease is usually accompanied by fever and marked prostration.
• It is also known that children are more frequently attacked than adult
persons and the symptoms are more severe.
20.
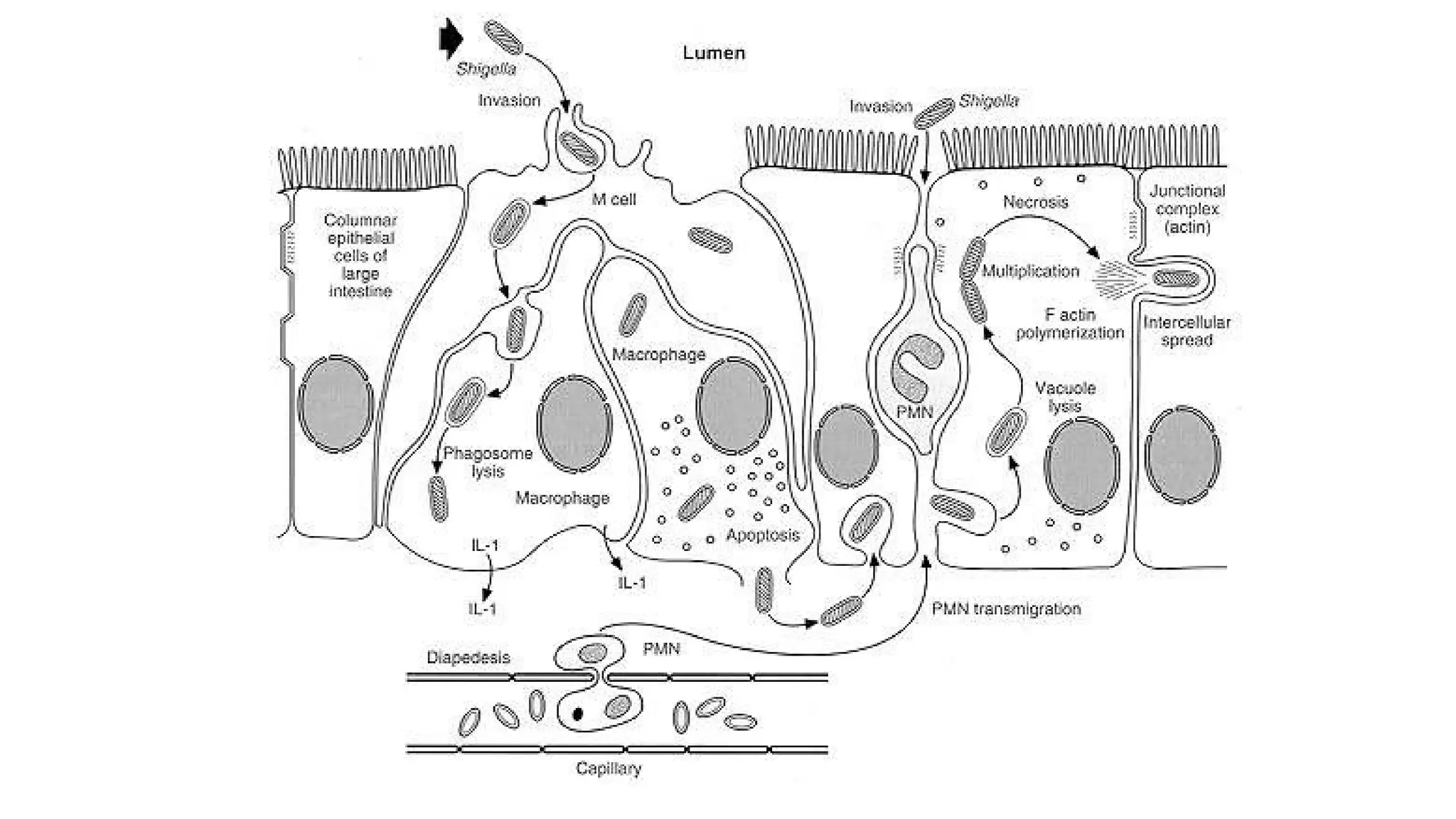
• Bacterial cellspreferentially attach to and invade into M cells in
Peyer’s patches (lymphoid tissue, i.e., lymphatic system) of small intestine.
• M cells typically transport foreign antigens from the intestine to
underlying macrophages,
• but Shigella can lyse the phagocytic vacuole (phagosome) and
replicate in the cytoplasm.
(Note: This contrasts with Salmonella which multiplies in the
phagocytic vacuole)
• Actin filaments propel the bacteria through the cytoplasm and into
adjacent epithelial cells with cell-to-cell passage, thereby effectively
avoiding antibody-mediated humoral immunity (similar to Listeria
monocytogenes).
22.
• Shigella areable to penetrate through mucosal surface of colon
(colonic mucosa) and invade and multiply in the colonic epithelium
but do not typically invade beyond the epithelium into the lamina
propria (thin layer of fibrous connective tissue immediately beneath the surface
epithelium of mucous membranes)
• Areas of intense inflammation developed around the multiplying
bacteria and micro abscesses form and spread leading to bleeding
ulceration.
• Bacteriaemia is very rare as their invasion is usually restricted
to mucosa membrane.
23.
• The symptomsincludes abdominal pain, fever and diarrhoea with
mucus and blood in excretion.
• Bacterial dysenteriae is normally a self limiting with recovering
occurring with in 2-7 days.
• The severe dehydration associated with this disease can cause shock
& may lead to death in very young & very old.
24.
Laboratory diagnosis
• canbe done by immediate isolation of the bacillus from faeces
obtained by rectal swab or fresh stool.
• The specimens should be transported in glycerol saline (never in
highly alkaline transport Cary Blair medium used for vibrio).
• Mucus flakes are preferred and can be inoculated on MacConkey agar
and DCA media.
• After incubating overnight at 37°C, pale colonies are tested for
motility and biochemical reactions.
• The identification is confirmed by slide agglutination with polyvalent
or monovalent sera.
• Identification of shigellae in faeces can also be done by fluorescent
antibody technique. Serodiagnosis is of no value.
25.
Treatment of Shigella:
•Oral rehydration therapy (ORT) is adequate in all uncomplicated
shigellosis cases.
• Routine antibacterial treatment is not indicated in dysentery because
of the multiple drug resistance of shigellae.
• However, antibodies are reserved for the severe toxic cases.
26.
Prevention and Controlof Shigella:
• Man is the main source of infection (bacillary dysentery).
• He may transmit dysentery bacilli by touching door handle of latrine
with the contaminated fingers.
• The disease may also be transmitted by contaminated food through
faeces and flies from person to person.
• The infection can be controlled by satisfactory sanitation along with
the detection and treatment of patients and carriers.












![Enterotoxic Effect:
• Adheres to small intestine receptors.
• Blocks absorption (uptake) of electrolytes, glucose, and amino acids
from the intestinal lumen
[Note: This contrasts with the effects of cholera toxin (V. cholerae) and labile toxin
(LT) of Enterotoxigenic E. coli (ETEC) which act by blocking absorption of Na+, but
-
also cause hypersecretion of water and ions of Cl-, K+ (hypokalemia), and HCO3
(loss of bicarbonate buffering capacity leads to metabolic acidosis) out of the
intestine and into the lumen]
Neurotoxic Effect:
• Fever and abdominal cramping are considered signs of neurotoxicity.](https://image.slidesharecdn.com/4shigella-251123124640-ad6f98a8/75/about-Shigella-along-with-laboratory-diagnosis-13-2048.jpg)