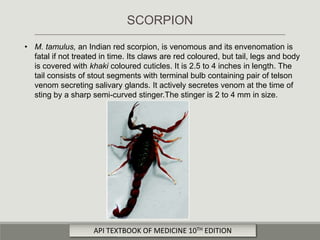
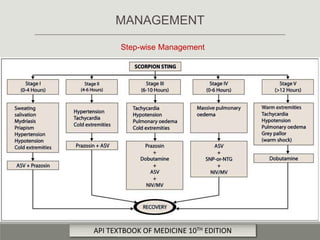
Scorpion stings are a major public health problem in tropical countries. The document discusses the clinical presentation, pathophysiology, grading, investigations, and management of scorpion stings. It focuses on the Indian red scorpion Mesobuthus tamulus, which can cause a life-threatening hypertensive crisis and pulmonary edema if not treated promptly. Prazosin is the primary treatment to counteract venom effects and prevent complications. Scorpion antivenom may also be given if autonomic symptoms persist. Supportive care includes fluid resuscitation, oxygen therapy, diuretics and inotropes as needed.