![• Classification and Risk Factors. Most commonly classified
based on the infecting pathogen and location at the onset
of illness.
• 1. Community-acquired meningitis. Patients have not been
recently hospitalized and/or undergone any recent
procedures (e.g., CSF shunt). Predisposing factors include
preexisting diabetes mellitus, otitis media, sinusitis,
pneumonia, and alcohol abuse. Pathogens can include
bacterial, viral, fungal, or parasitic agents.
• 2. Nosocomial meningitis and ventriculitis. Most commonly
related to infections associated with CSF shunts, CSF drains,
intrathecal drug therapy, deep brain stimulation hardware,
neurosurgery procedures, and head trauma. Also usually
associated with a typical nosocomial bacterial pathogen
(e.g., methicillin-resistant Staphylococcus aureus [MRSA] or
vancomycin-resistant Enterococcus spp)](https://image.slidesharecdn.com/case7viralmeningitis-220512152315-9911cedb/85/Case-Presentation-On-Viral-Meningitis-9-320.jpg)


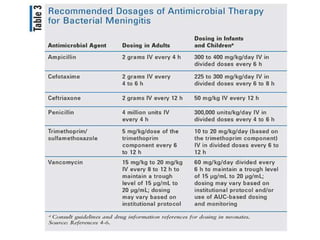

This case presentation discusses a 24-year-old female patient admitted with complaints of fever, altered sensorium, headache, and body pains. Examination found increased white blood cell count in cerebrospinal fluid analysis consistent with viral meningitis. The patient was treated with acyclovir and other supportive medications and showed improvement over time. The document then reviews causes, presentation, diagnostic testing, and treatment approaches for viral and bacterial meningitis.














































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)








