Downloaded 1,758 times


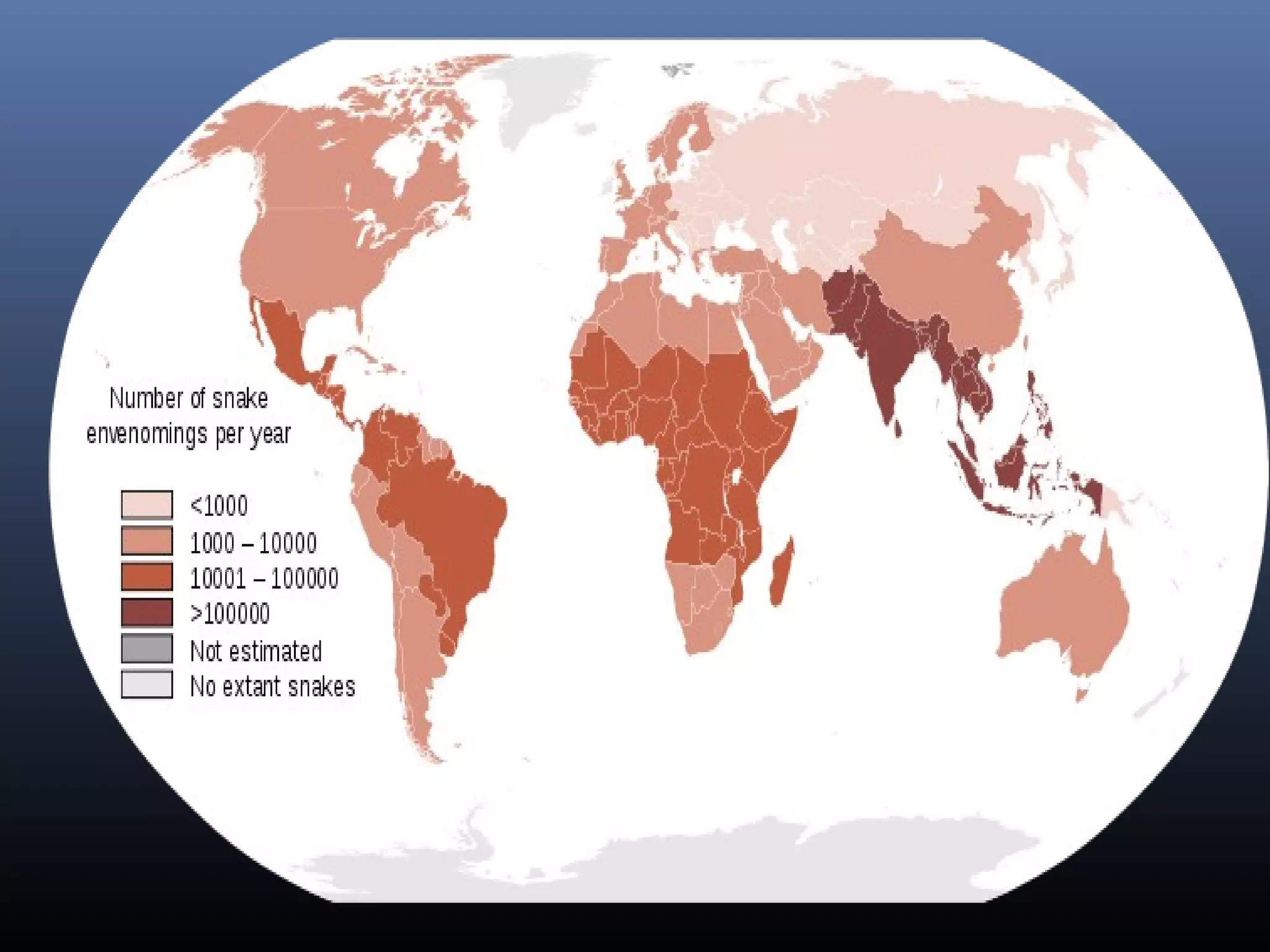









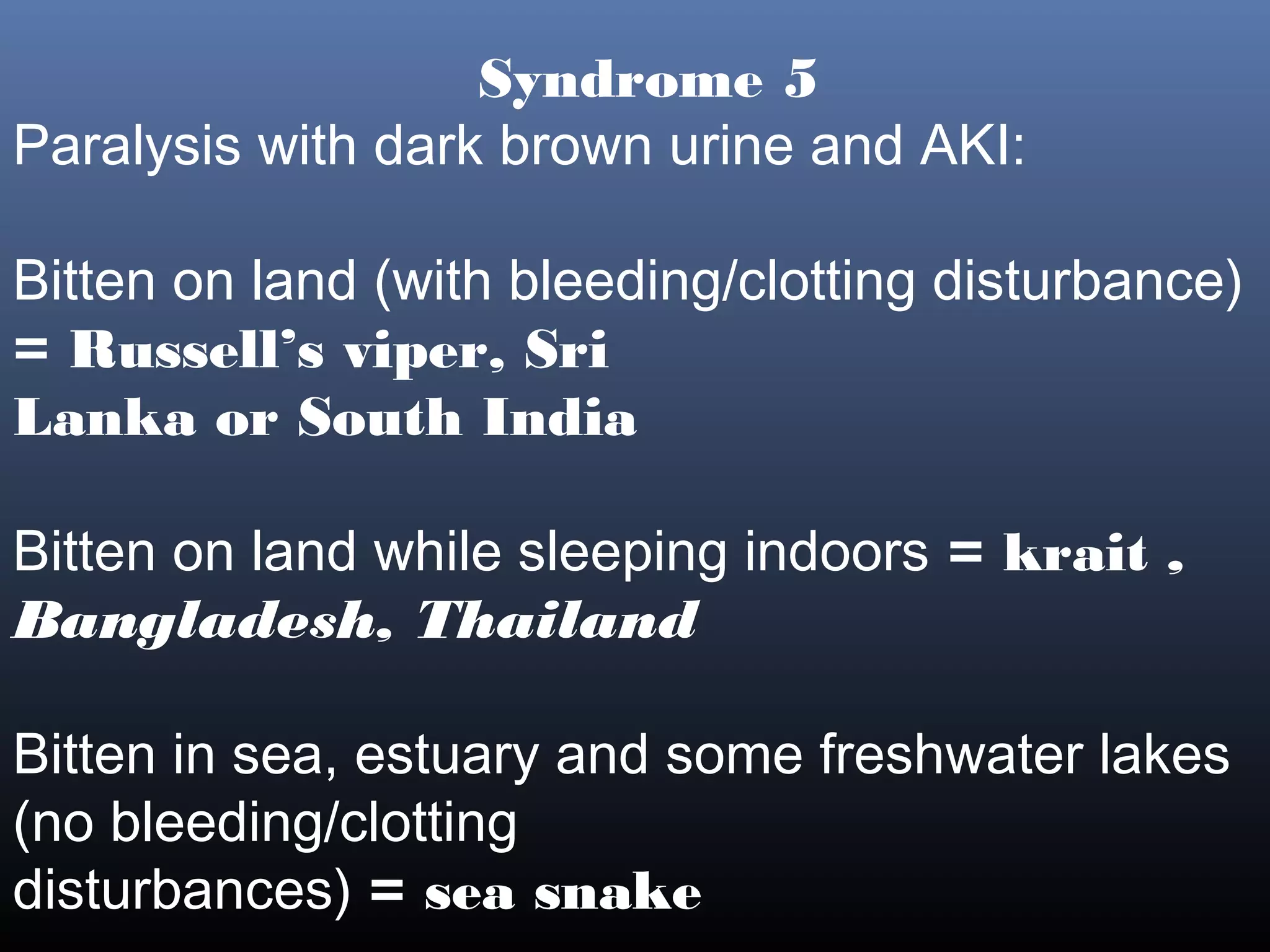
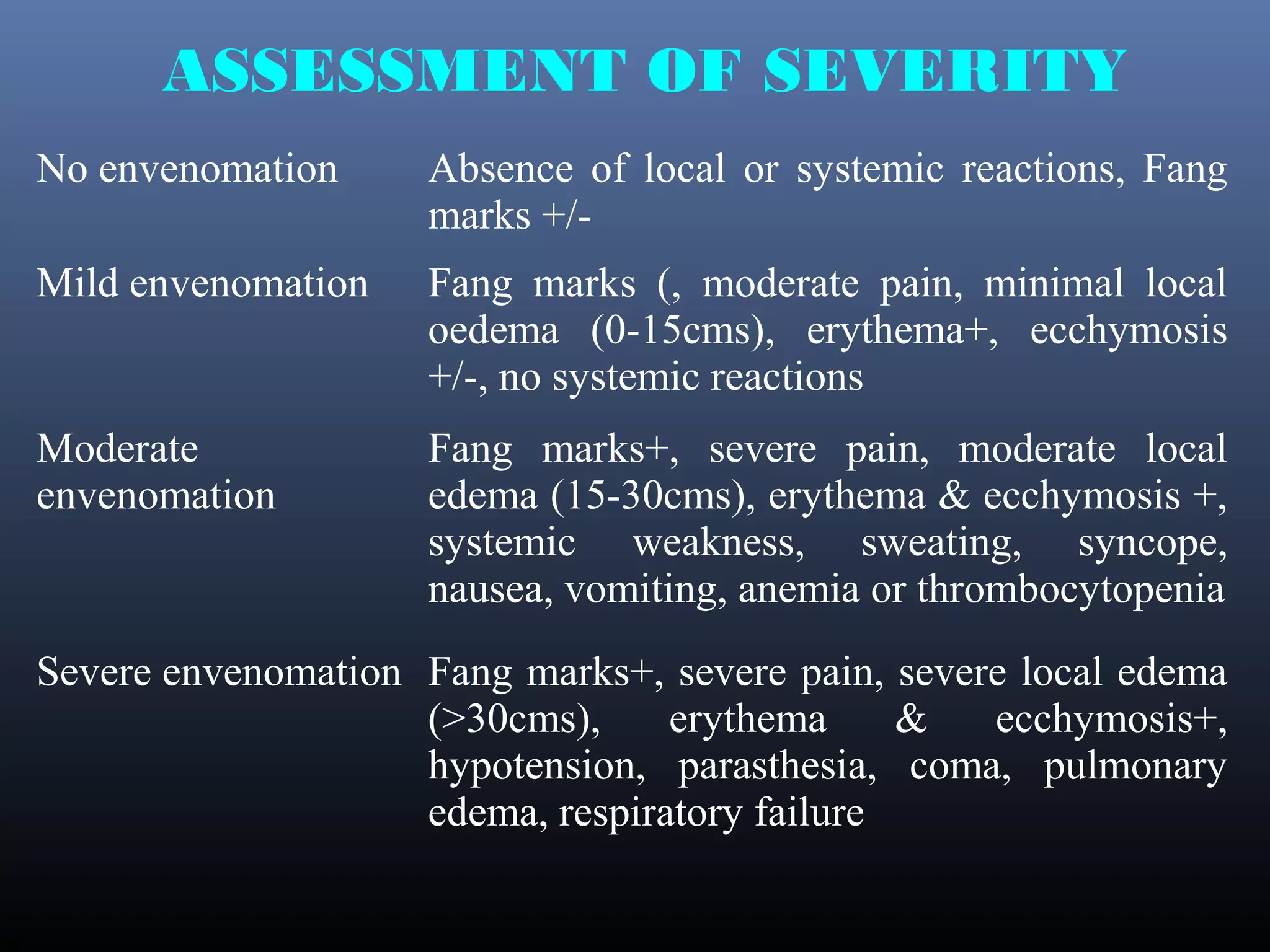
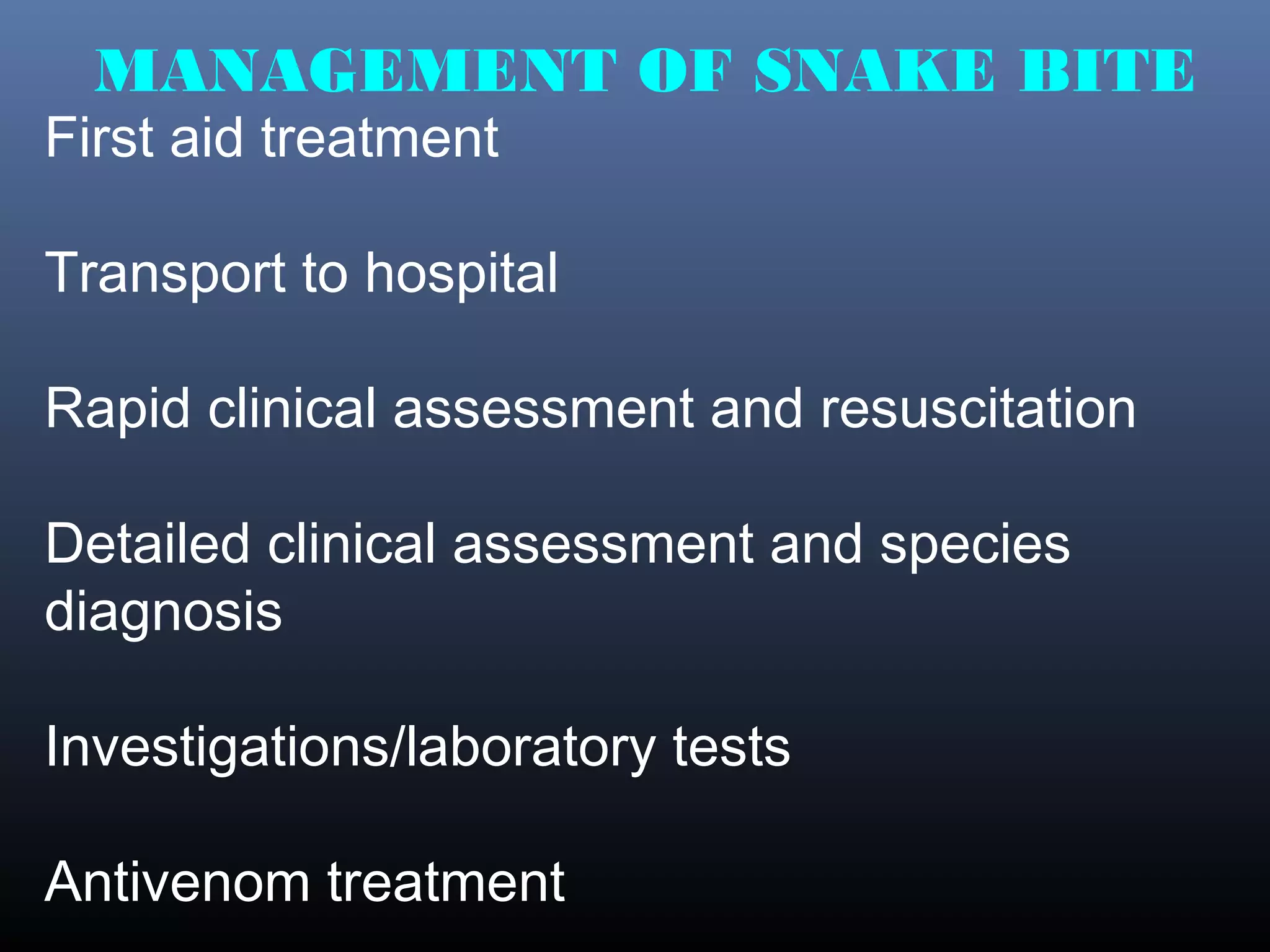
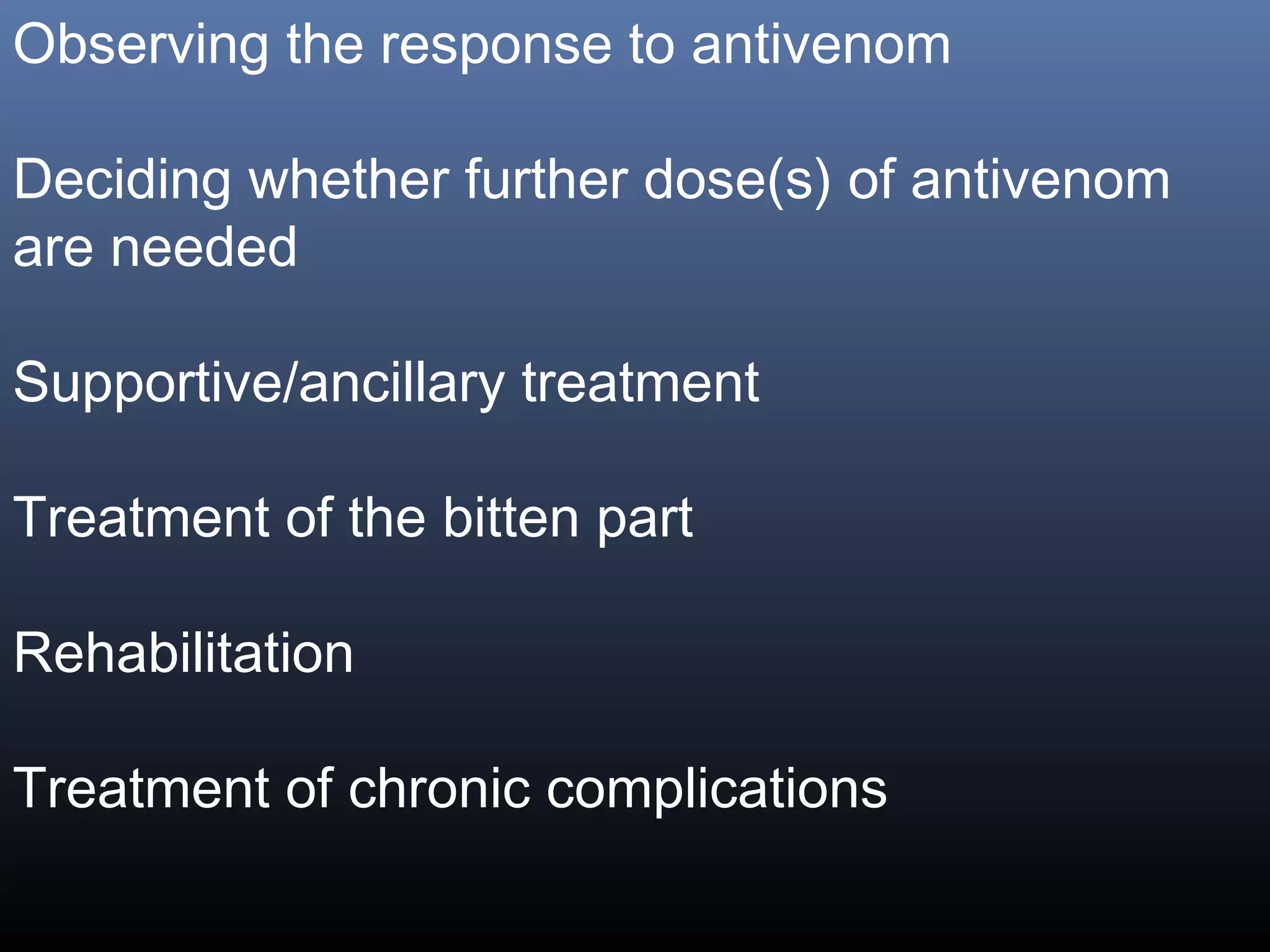


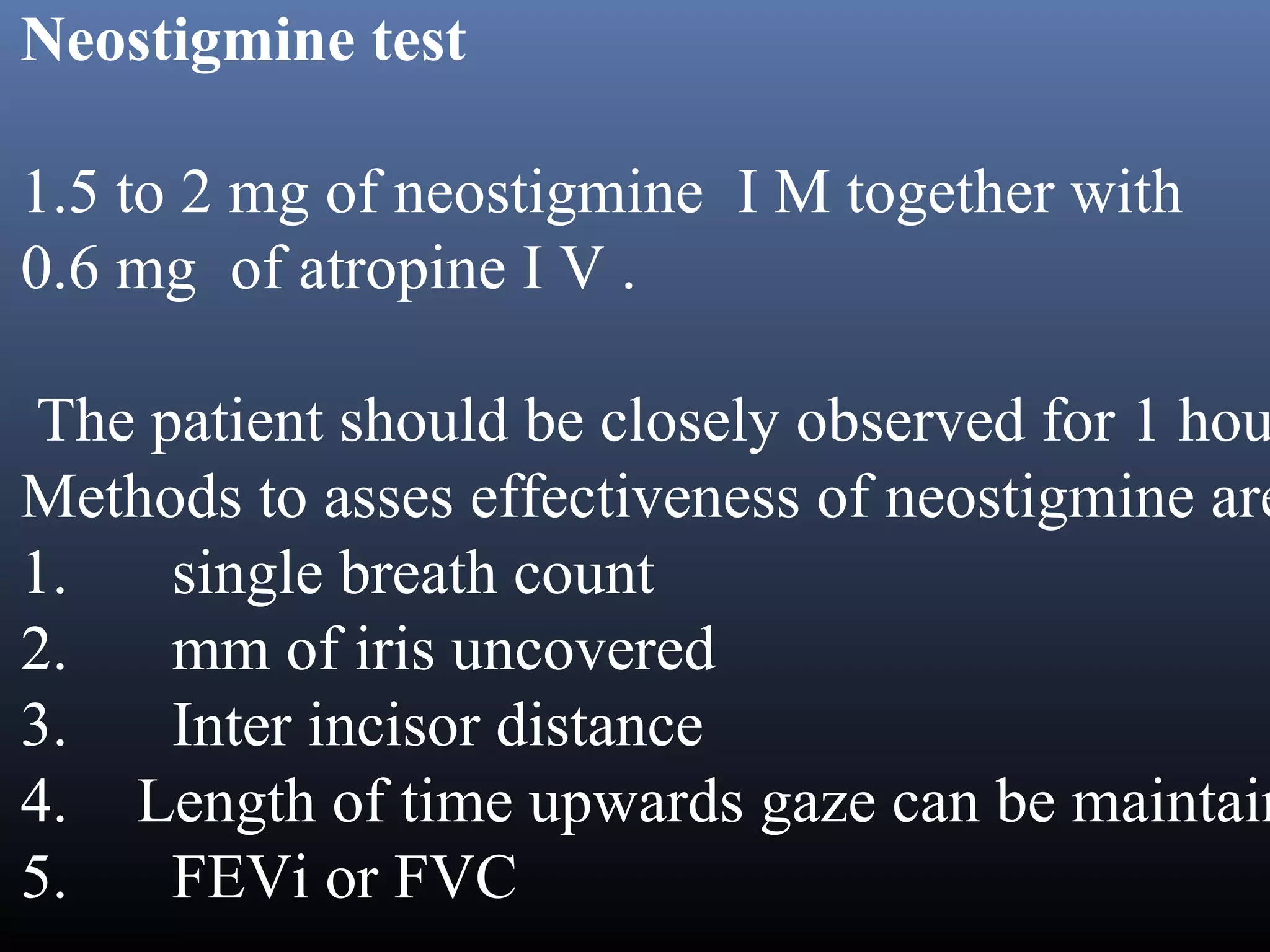

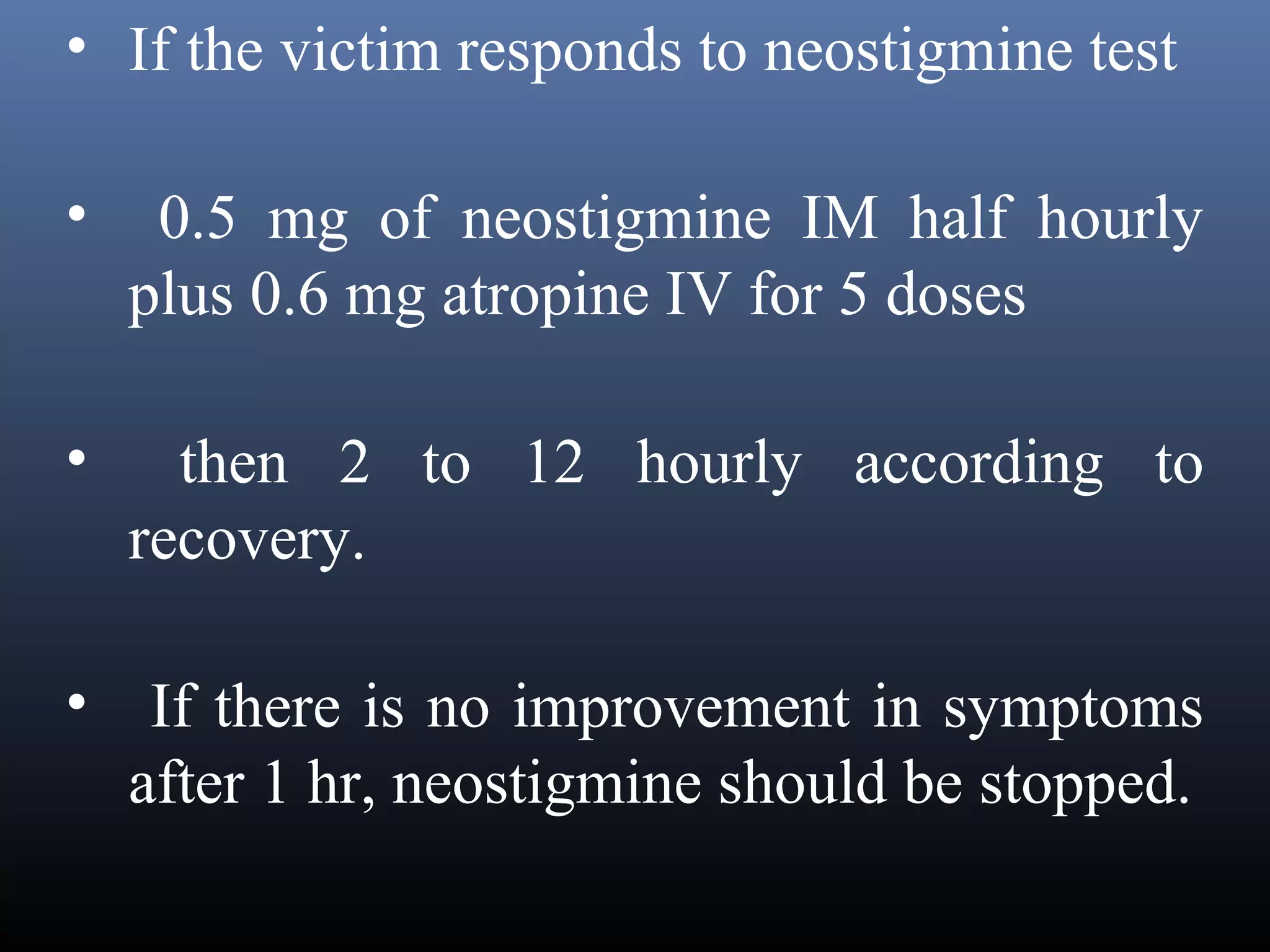
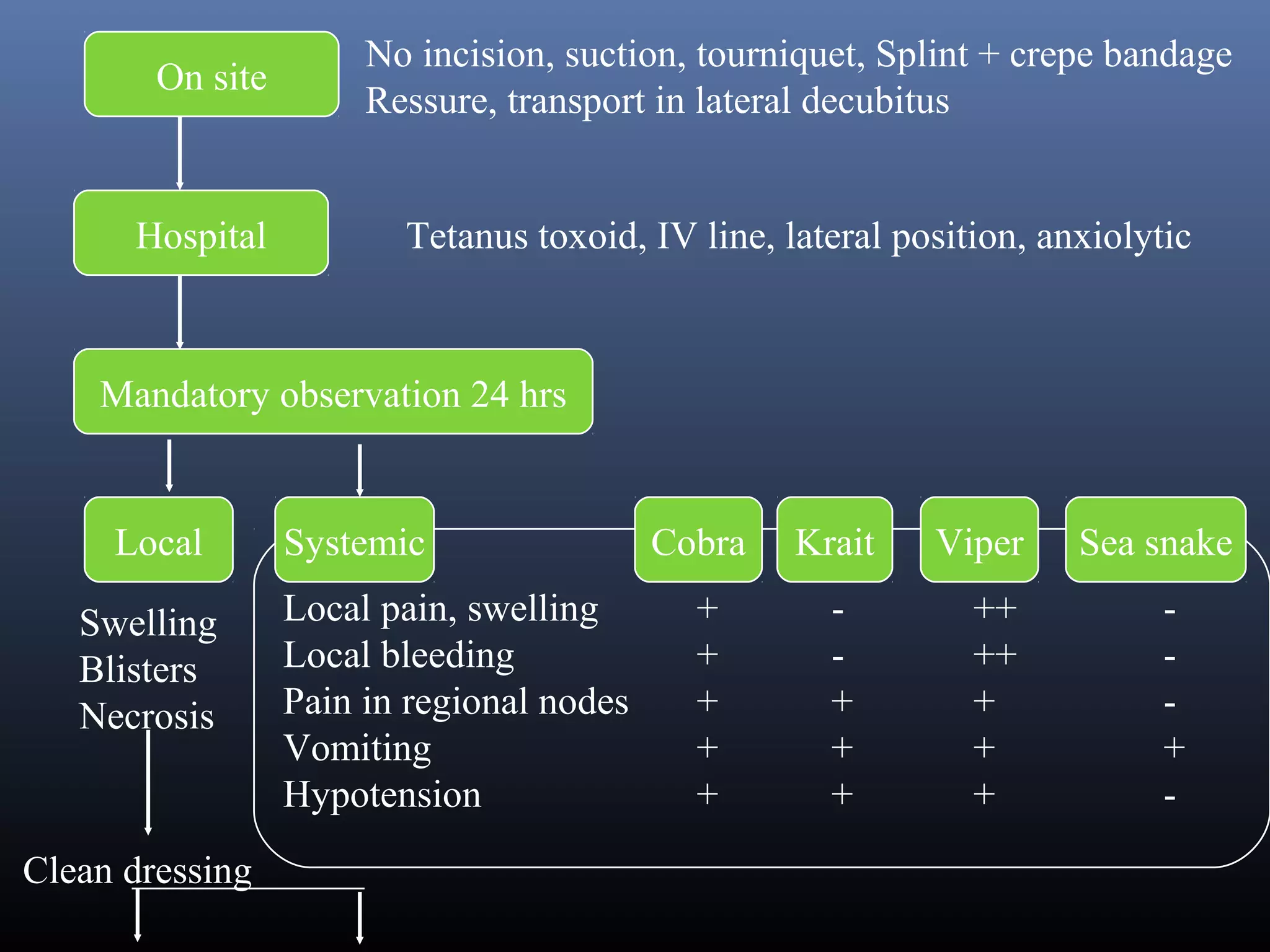
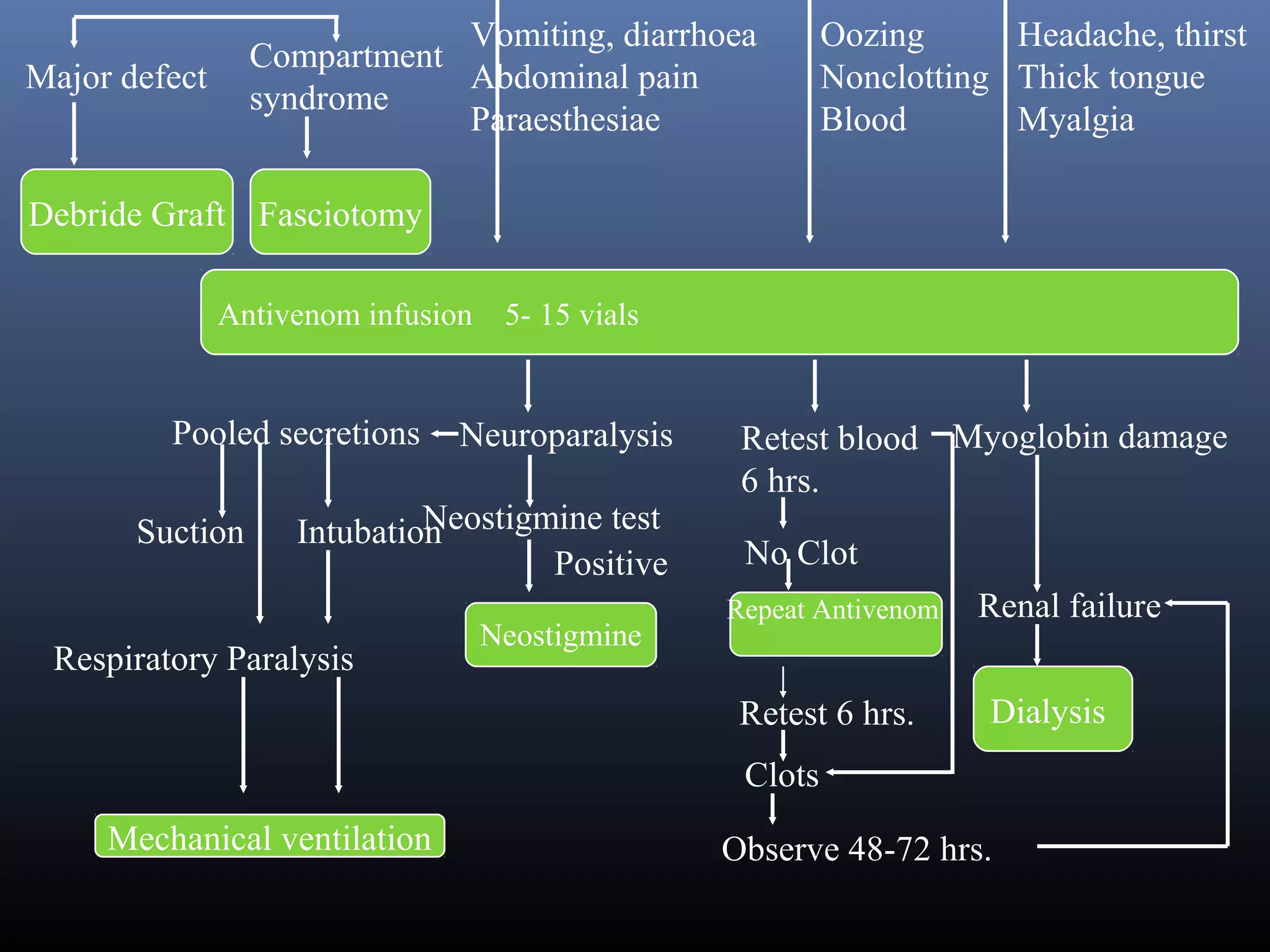


This document provides an extensive overview of snake bite management, highlighting the prevalence of snake bites in India and the various species of venomous snakes. It details the symptoms, signs, and complications associated with snake bites, along with treatment protocols including first aid, antivenom administration, and supportive care. The document emphasizes the importance of rapid assessment and intervention in snake bite cases to prevent severe outcomes.











































































































