Downloaded 153 times

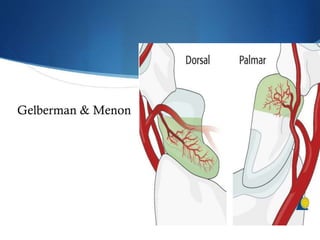
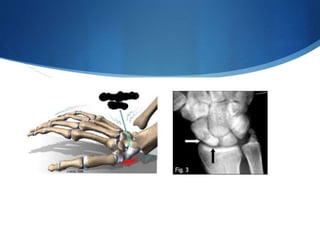
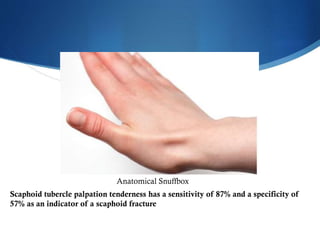

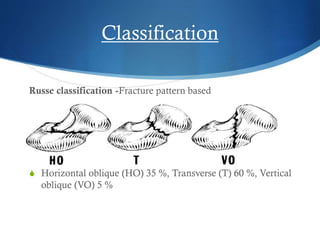

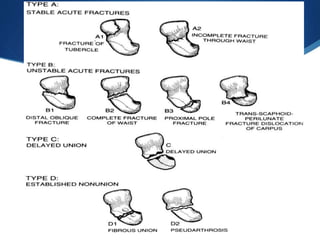
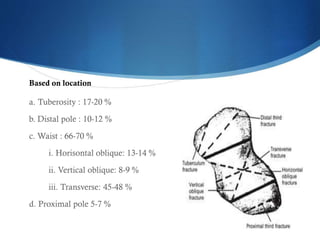
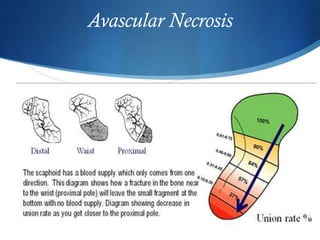
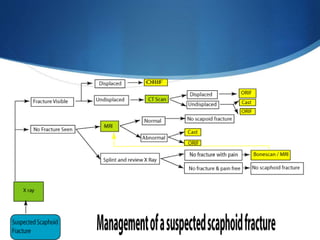

The scaphoid bone forms the radial part of the wrist and is susceptible to fractures due to its oblique orientation crossing two rows of carpus bones. It receives its blood supply from three main arterial groups. Common mechanisms of injury involve falls onto outstretched hands and forced wrist motions. Clinical evaluation for scaphoid fractures includes wrist pain, swelling over the anatomical snuffbox, and tenderness over the scaphoid tubercle. While initial x-rays may not detect up to 25% of fractures, other imaging like bone scans, MRI, CT, and ultrasound provide higher sensitivity. Fractures are classified based on location and displacement, with displaced fractures or those in the proximal pole requiring operative treatment














































































