Downloaded 187 times
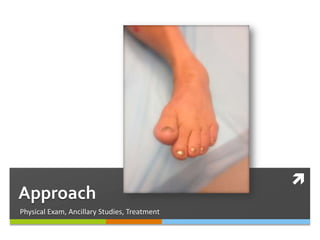




This document discusses subtalar dislocations, including: - There are four main types - medial, lateral, posterior, and anterior. Medial dislocations are most common. - Mechanisms of injury vary but often involve high-energy trauma like motor vehicle accidents or falls. Associated injuries are common. - Treatment involves closed or open reduction depending on the situation, followed by immobilization for 4-6 weeks. - Prognosis depends on factors like time to reduction and associated injuries. Most patients regain good function but arthritis and stiffness are common long-term.










































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















