Downloaded 12 times



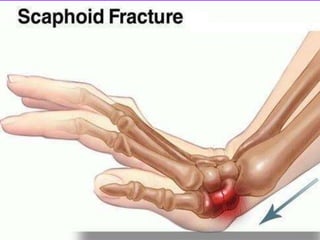



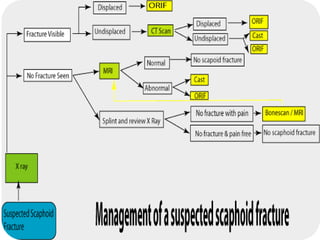


The document provides information about scaphoid fractures, including: - Scaphoid fractures most commonly occur at the waist portion of the bone and account for 50-80% of all carpal bone fractures. - Diagnosis is based on history, clinical examination showing tenderness over the scaphoid, and imaging including x-rays and advanced imaging if needed. - Treatment depends on fracture displacement and location, with nondisplaced fractures often treated non-operatively with casting and displaced or proximal fractures often requiring surgery. - Prognosis depends on factors like timing of diagnosis, location, displacement, and smoking, with proximal fractures having higher risks of complications like nonunion.






























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




