This document provides an overview of carpal instability, including:
1) Carpal instability occurs when an injury to a carpal ligament renders the wrist unstable as the carpal bones no longer move together properly.
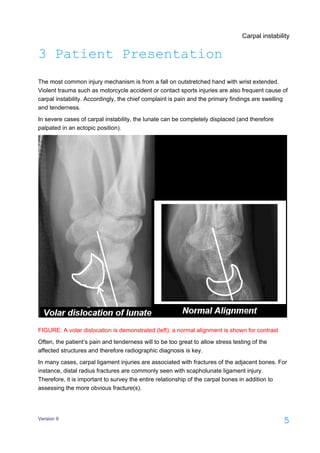
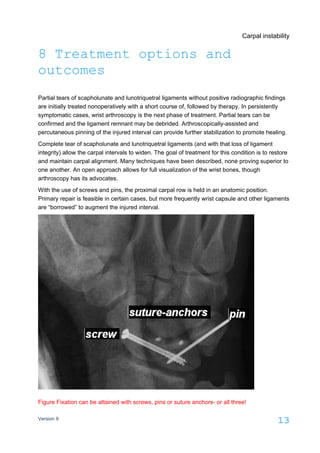
2) Clinical presentation includes pain with wrist motion and tenderness over ligaments. Imaging can detect abnormal bone positioning or arthritis. Arthroscopy is the gold standard for diagnosis.
3) Risk factors include falls on an outstretched hand or high-energy trauma. Differential diagnosis includes tendonitis and nerve issues. Red flags include persistent pain after fracture healing or neurologic symptoms.