Downloaded 73 times
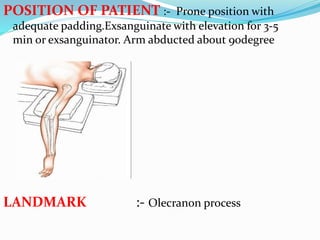
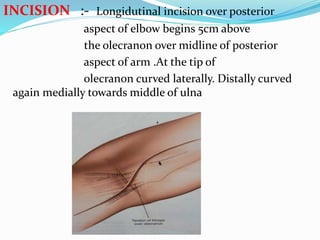

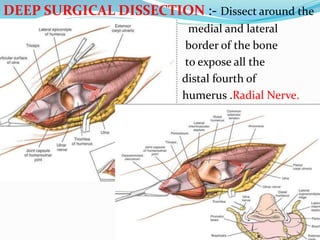
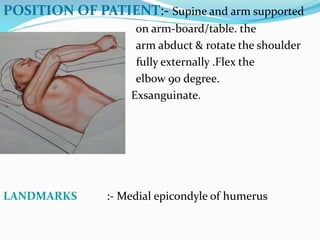
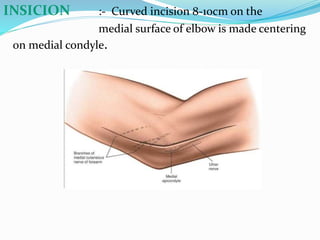
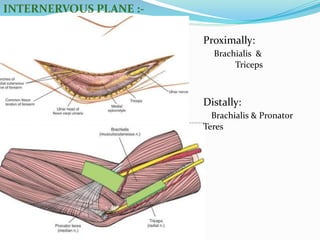
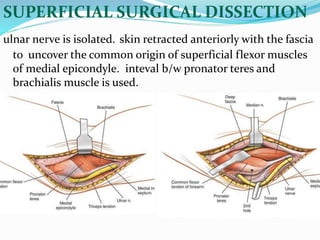
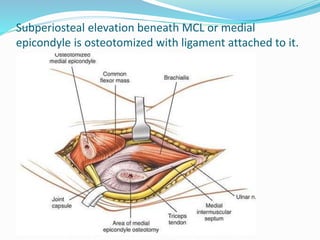
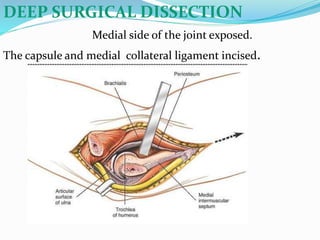
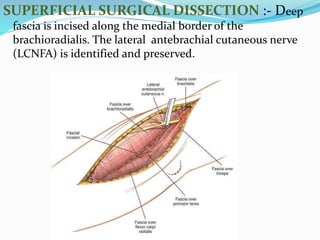
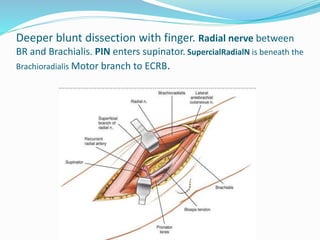
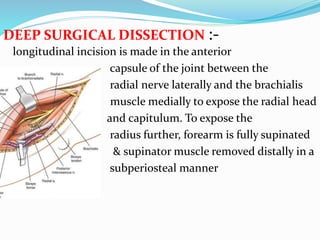
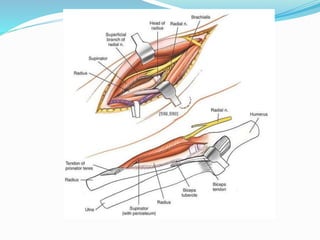
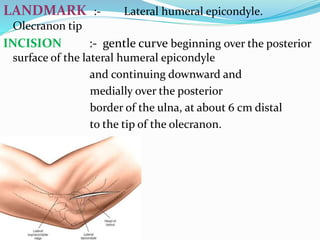
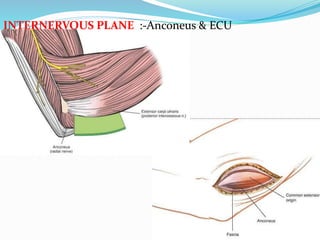
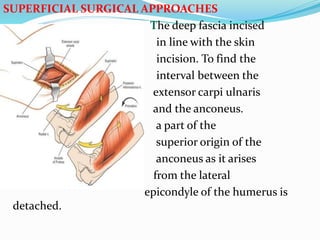
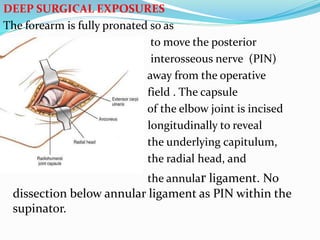

This document describes various surgical approaches to the elbow, including the posterior, medial, anterolateral, anterior of cubital fossa, and posterolateral approaches. For each approach, it provides the indications, patient positioning, landmarks, incision details, internervous planes, superficial and deep dissections, and structures at risk. The posterior approach is used for fractures of the distal humerus. The medial approach provides access to the medial condyle and coronoid process. The anterolateral approach is used for fractures of the radial head and capitellum.













































































