Downloaded 123 times
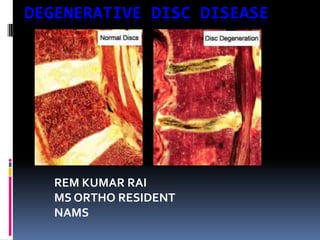
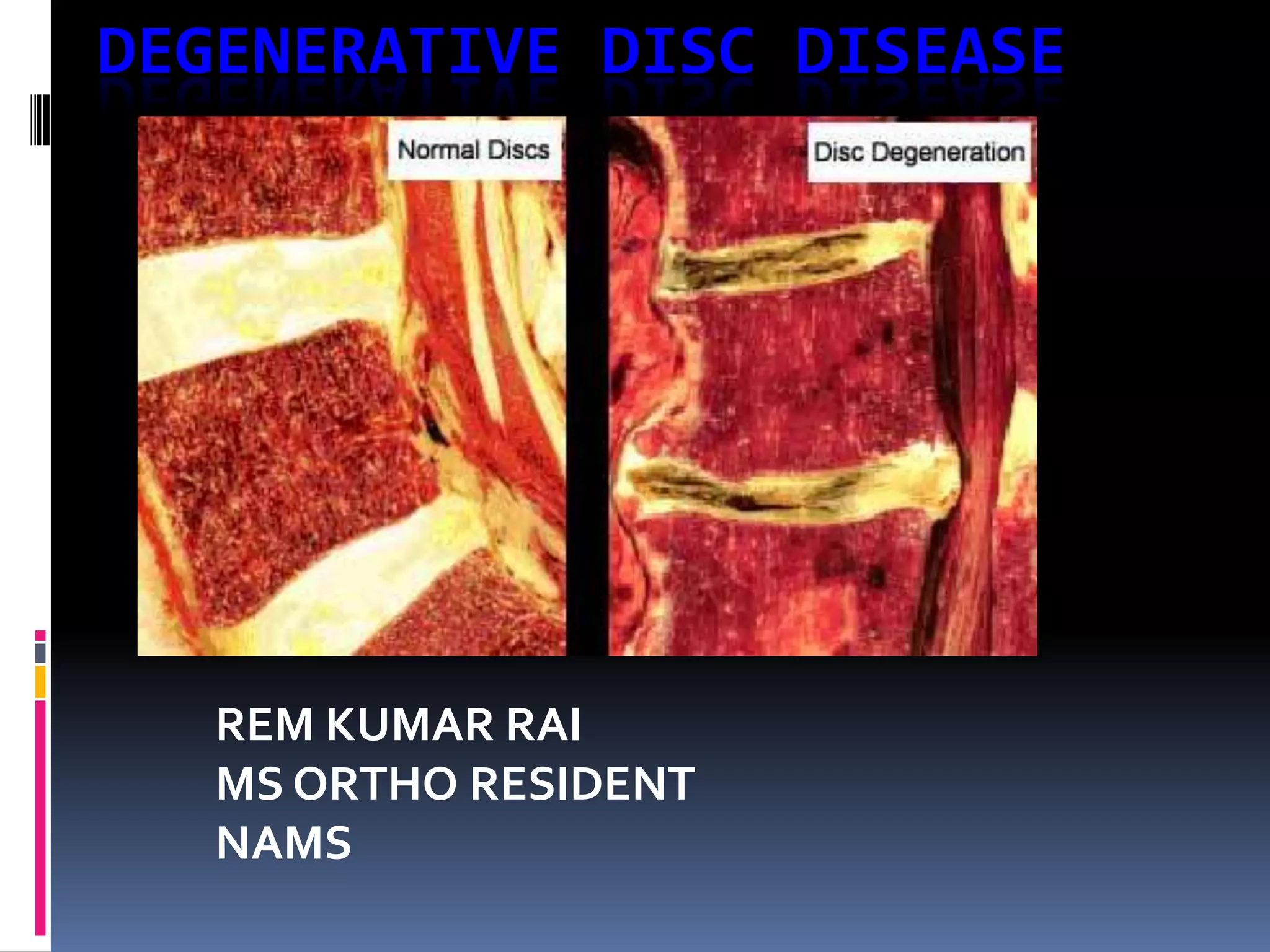
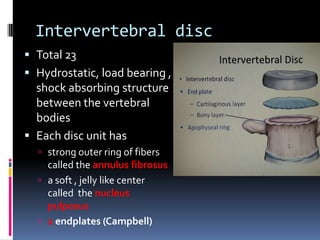
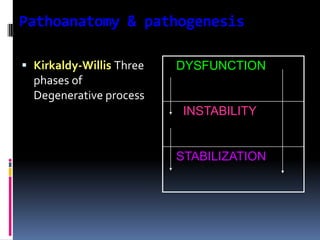
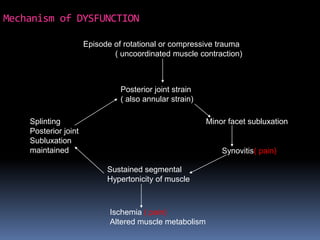
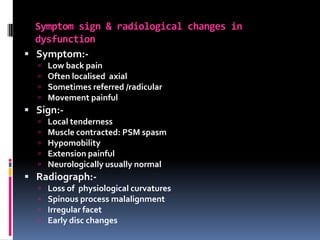
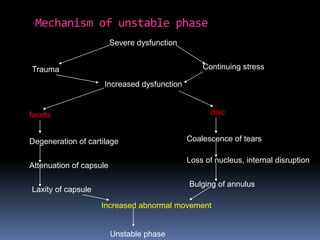
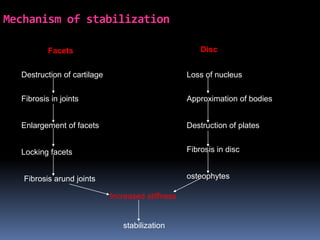
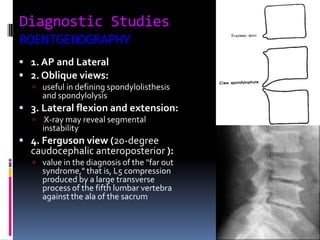
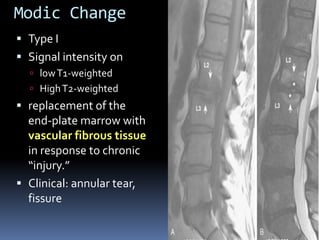
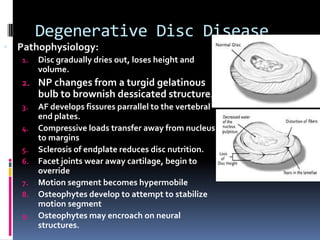
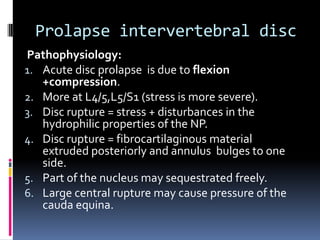
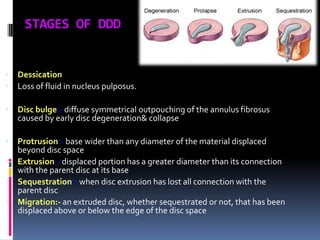
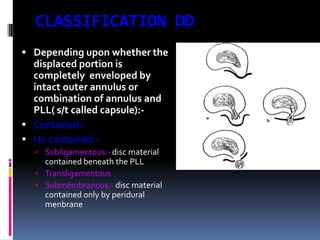
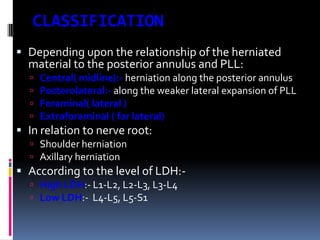


Degenerative disc disease is a condition characterized by changes in the discs between vertebrae. As discs degenerate they lose water content and height. Fissures can form in the annulus fibrosus and the nucleus pulposus loses structure. This can lead to bulging of the disc and potentially protrusion or extrusion of disc material. Kirkaldy-Willis divided the process into three stages: dysfunction, instability, and stabilization. Symptoms include back pain and pain that may radiate into the legs. Diagnostic imaging includes x-rays, CT, MRI, and discography which can help identify problematic discs.











































































