Downloaded 100 times
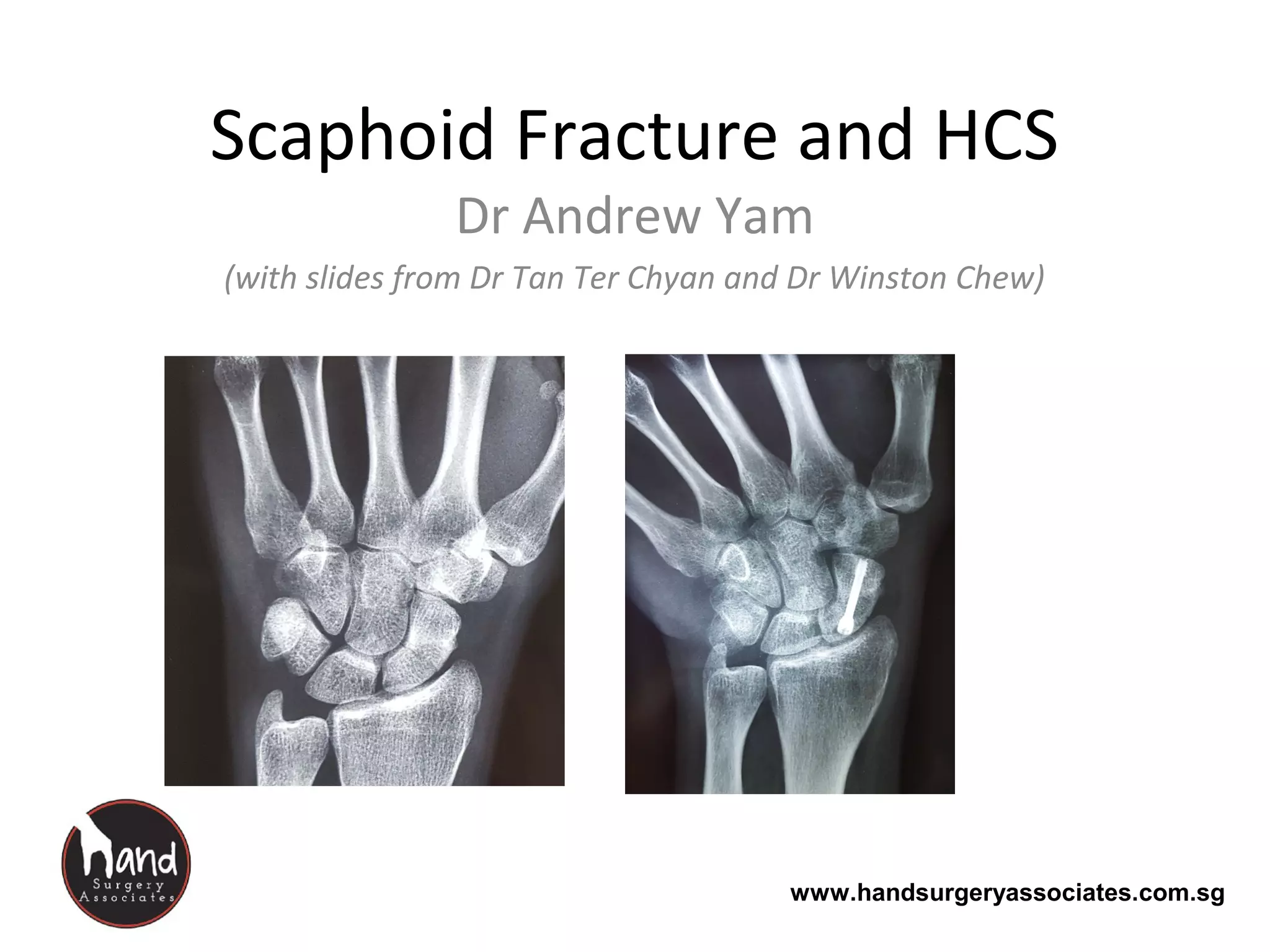

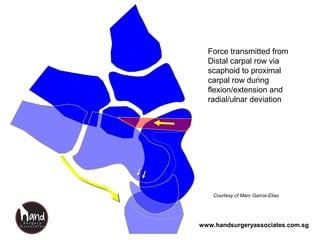
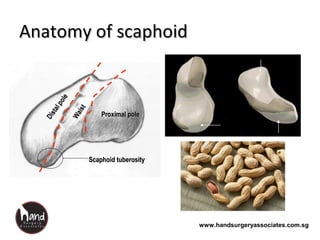
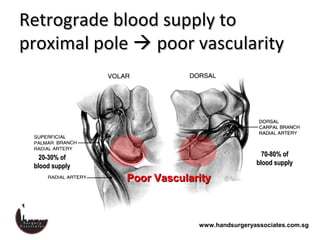
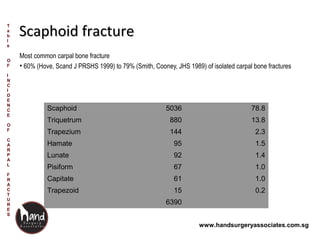
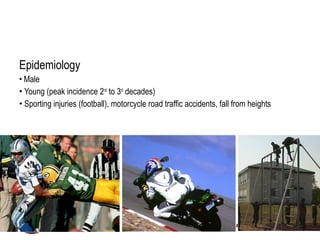
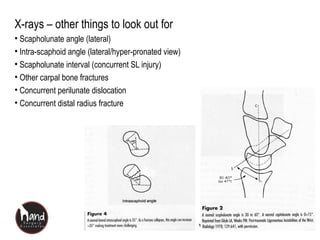
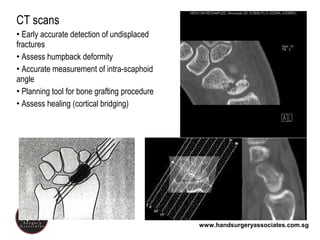
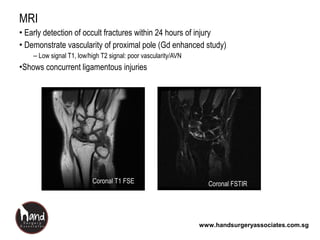
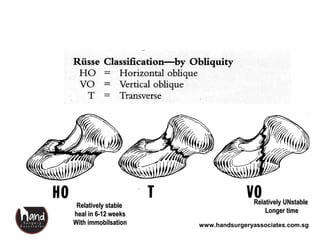
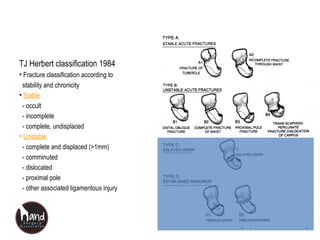
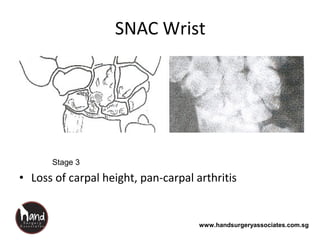
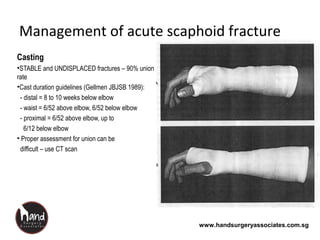
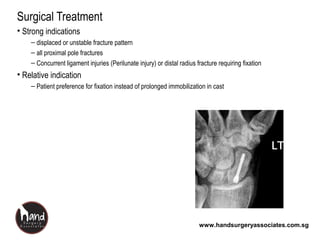

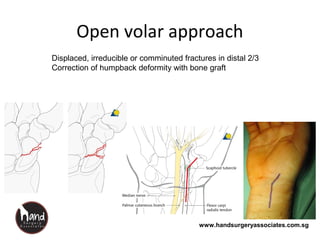
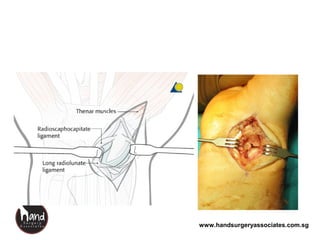
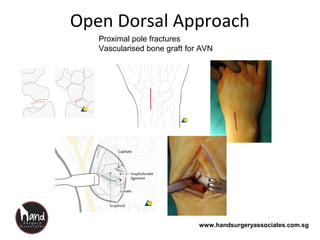

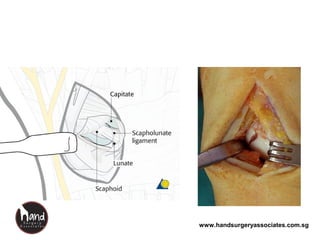
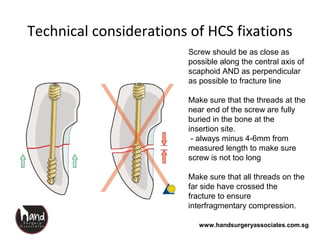
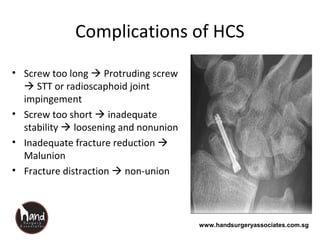
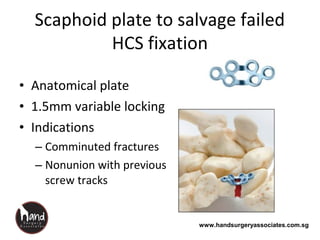
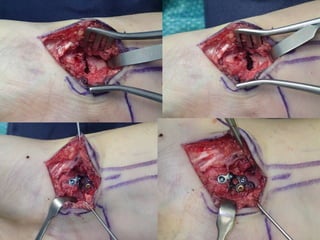



This document discusses scaphoid fractures, including the anatomy and blood supply of the scaphoid bone, mechanisms and epidemiology of scaphoid fractures, methods of diagnosis including x-rays, CT scans and MRI, classification systems, nonunion risks, and management approaches including casting, percutaneous screw fixation, and plate fixation. It focuses on the role of headless compression screw fixation for acute scaphoid fractures and its advantages over casting for earlier return to function and lower nonunion rates. Complications of screw fixation and salvage options for failed screw fixation using a scaphoid plate are also reviewed.























































































