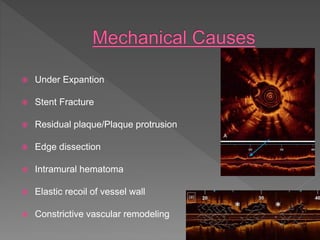
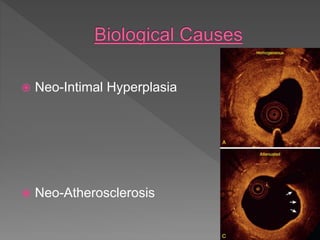
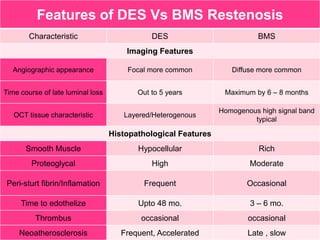
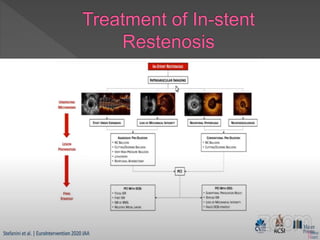
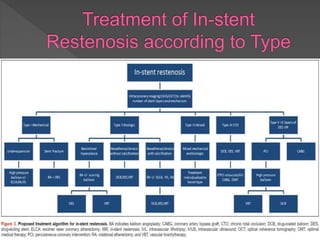
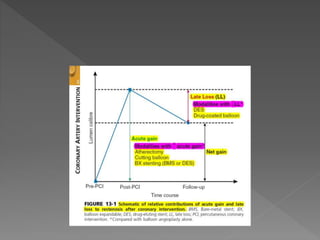
The document discusses definitions and etiology of in-stent restenosis as well as treatments for it. It defines angiographic, IVUS/OCT, and pathological definitions of restenosis. It also discusses the causes of in-stent restenosis including mechanical factors like underexpansion and biological factors like neointimal hyperplasia. The document then summarizes various treatment strategies for in-stent restenosis such as plain balloon angioplasty, atherectomy, brachytherapy, repeat stenting, and drug-coated balloons. It provides details on studies comparing the effectiveness of these different treatment methods.