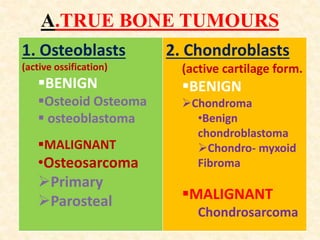
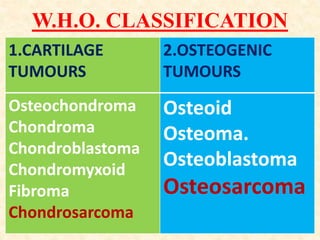
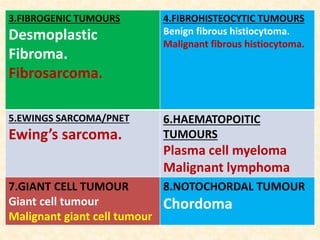
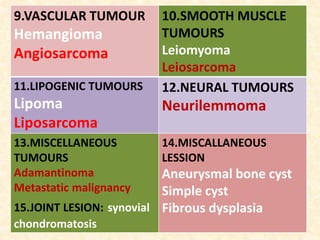
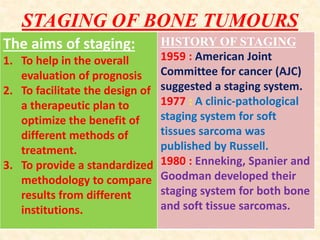
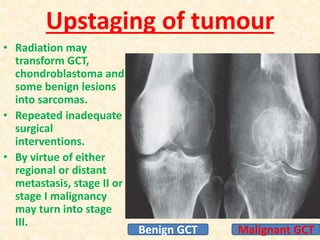
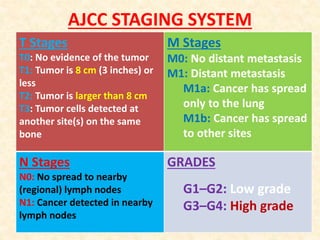
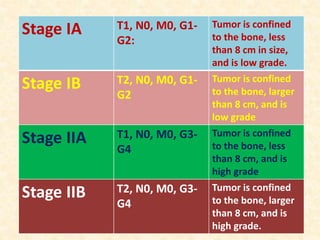
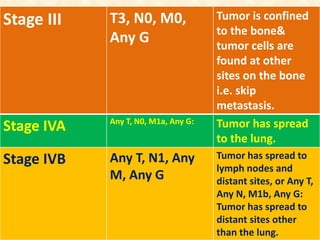
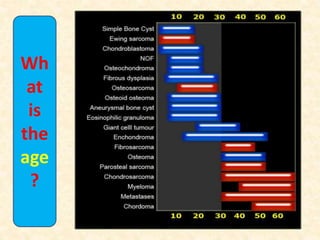
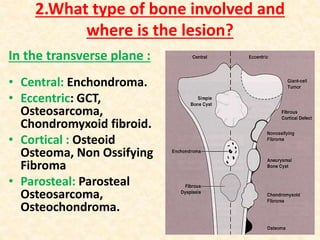
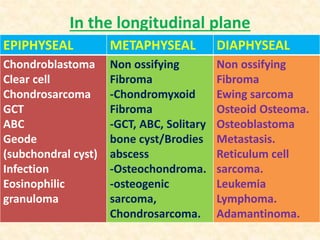
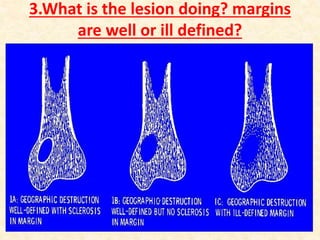
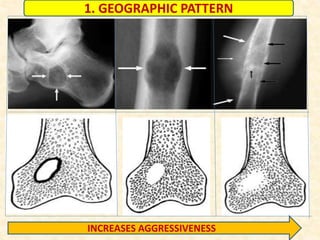
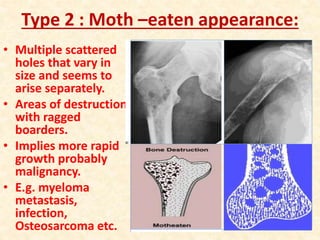
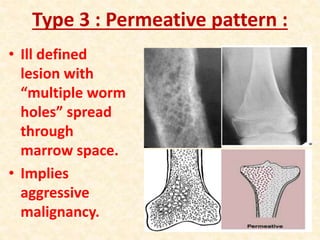
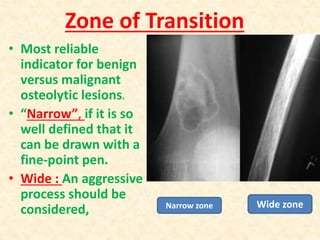
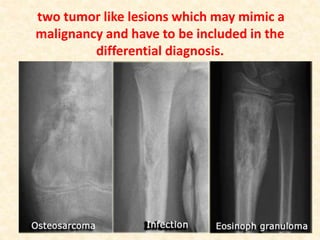
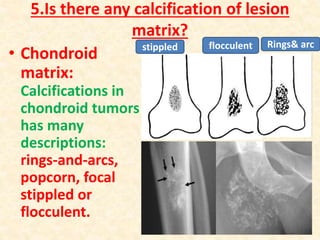
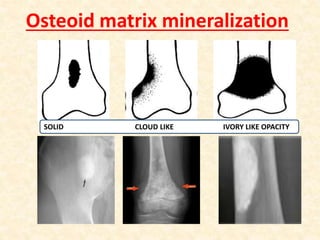
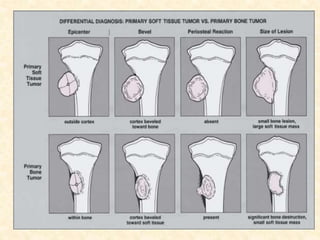
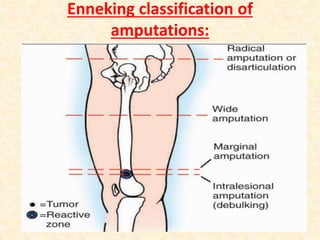
This document discusses the classification, investigations, and general management of bone tumors. It begins with definitions of tumors and then covers various classification systems for bone tumors including the Duthie-Belhobek-Mark system and WHO classification. Key points of each classification are described. The document also discusses staging of bone tumors using the Enneking and AJCC systems. Common investigations for bone tumors including plain x-rays are outlined. X-ray findings that can help determine the aggressiveness of tumors are described.