This document discusses calcium metabolism and homeostasis. It notes that calcium levels are tightly regulated by the intestine, kidneys, bones, and hormones. The parathyroid hormone (PTH) increases calcium absorption from the intestine and bones while decreasing urinary calcium excretion. Vitamin D increases intestinal calcium absorption. Calcitonin decreases bone resorption. Together, these organs and hormones work to maintain calcium levels within a narrow range. Imbalances can lead to hypo- or hypercalcemia with various neurological, cardiac, and musculoskeletal symptoms.








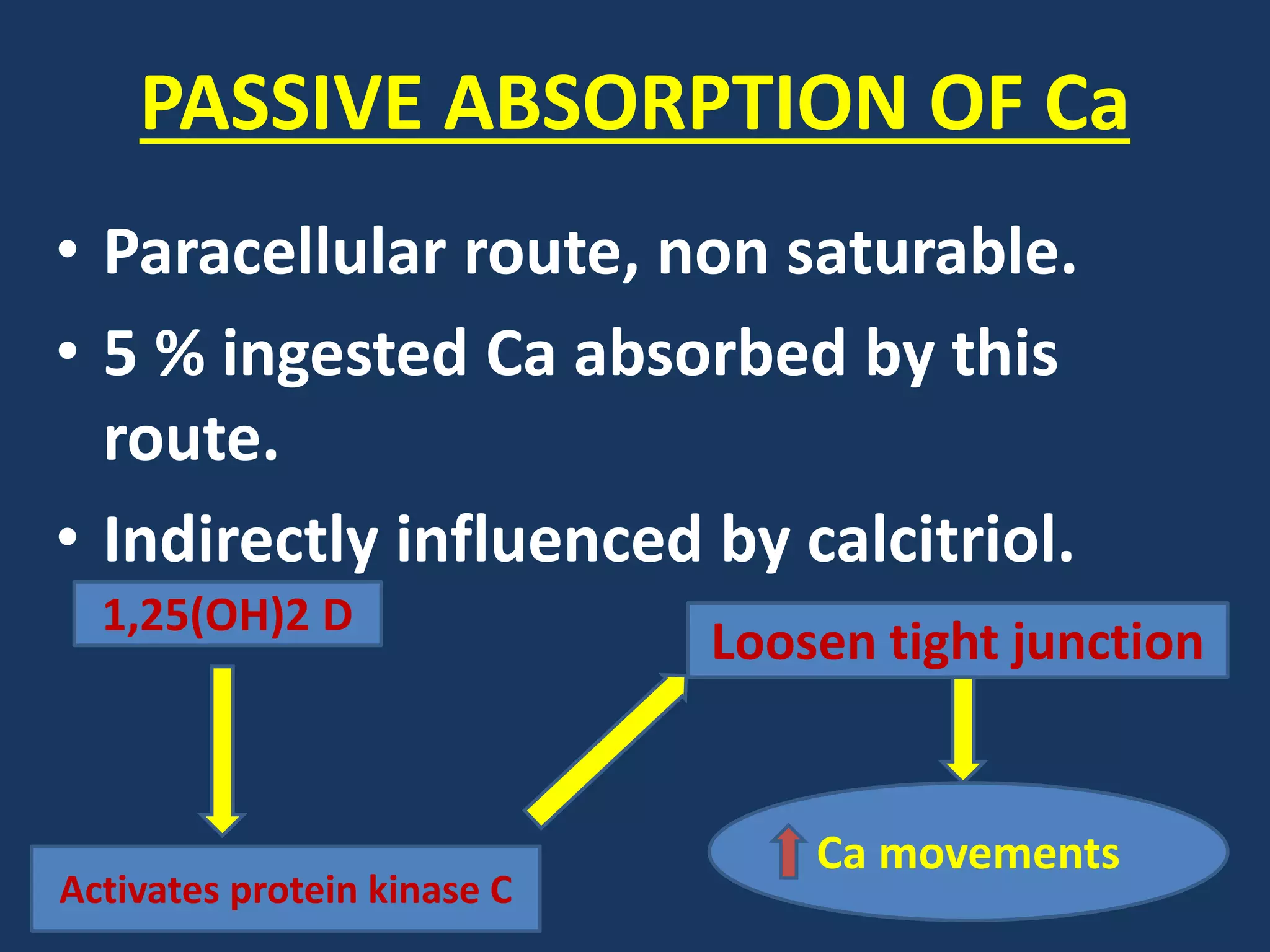







![Cont..
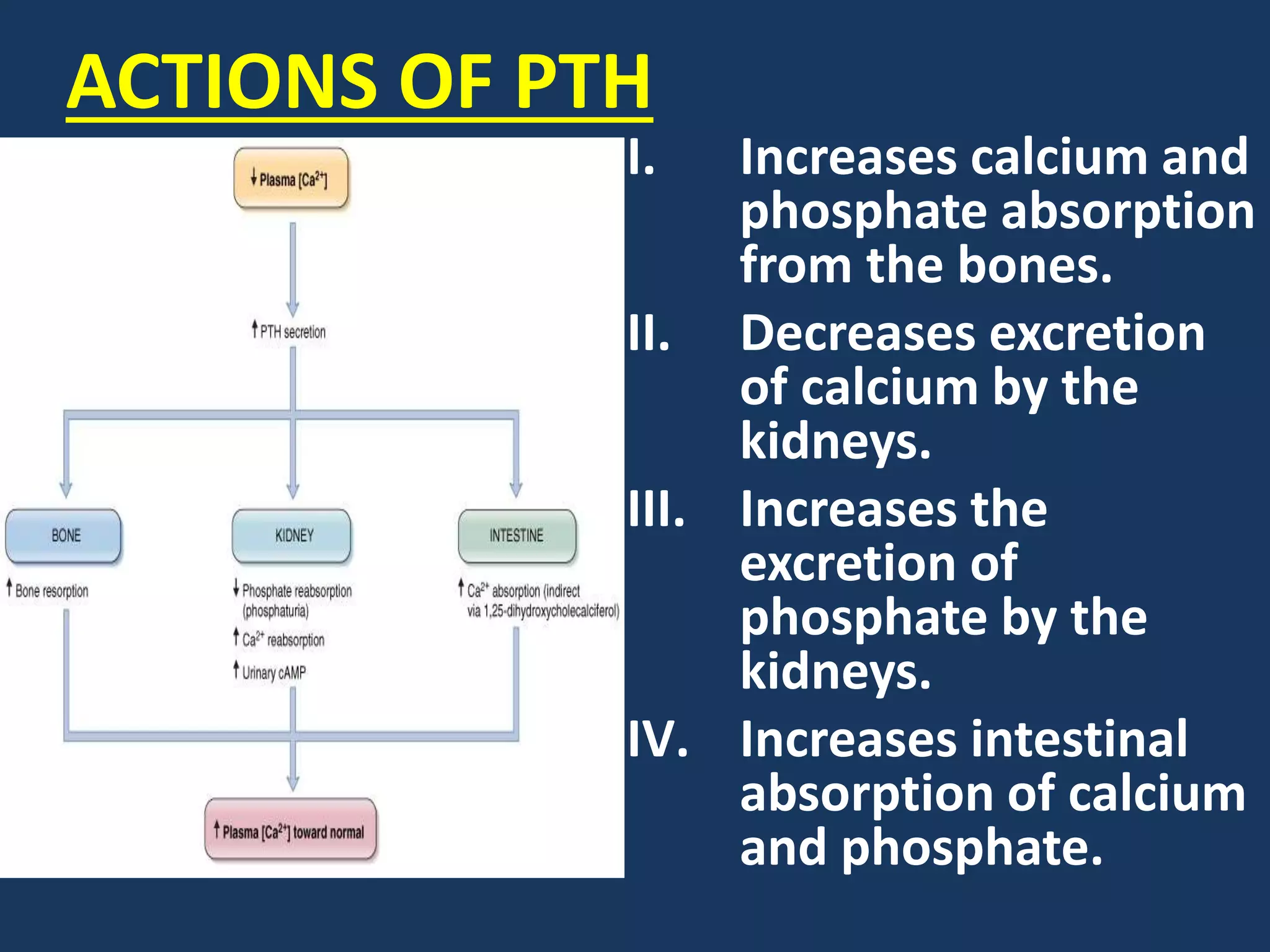
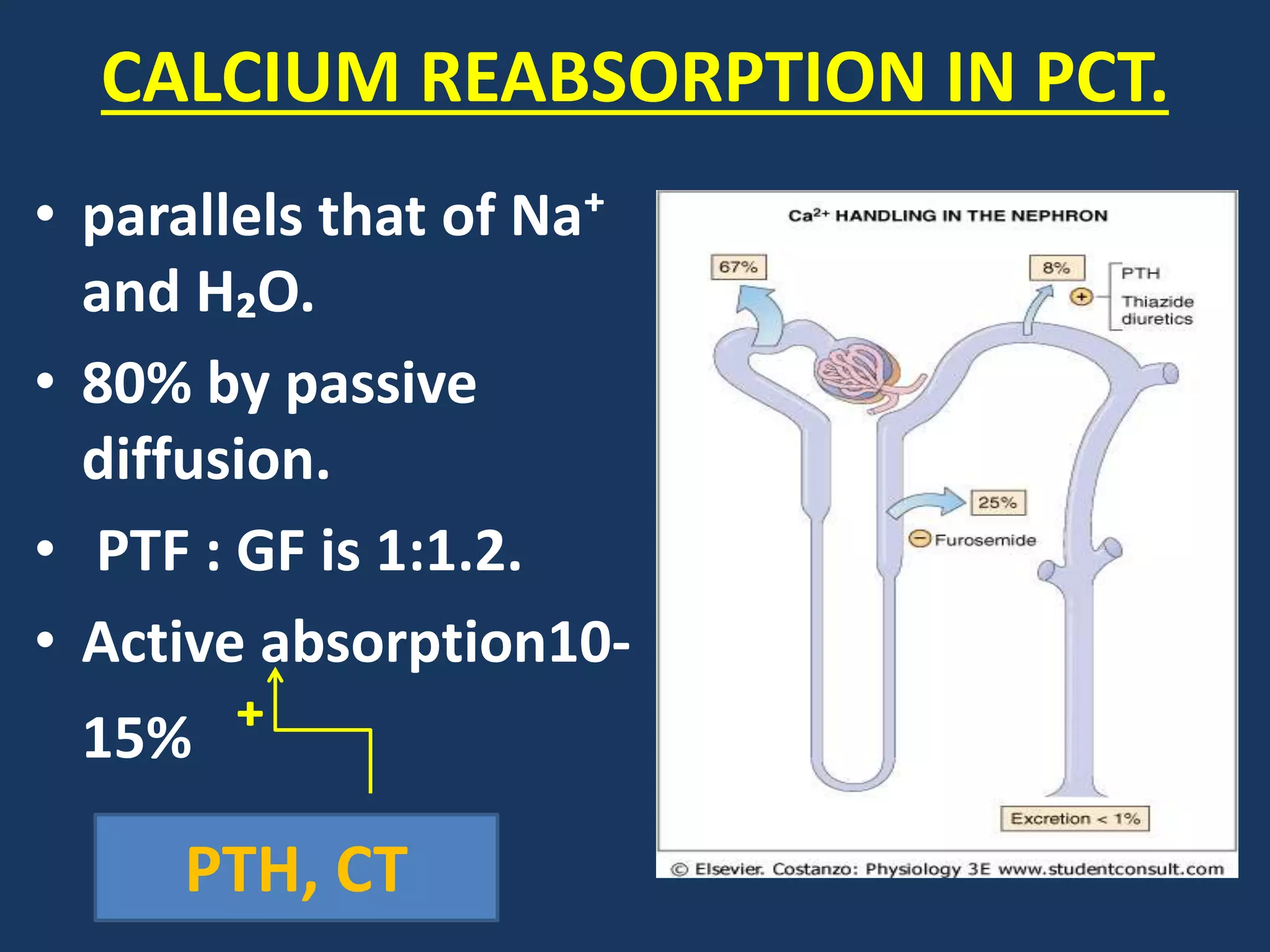
• PTH and CT
stimulate calcium
absorption.
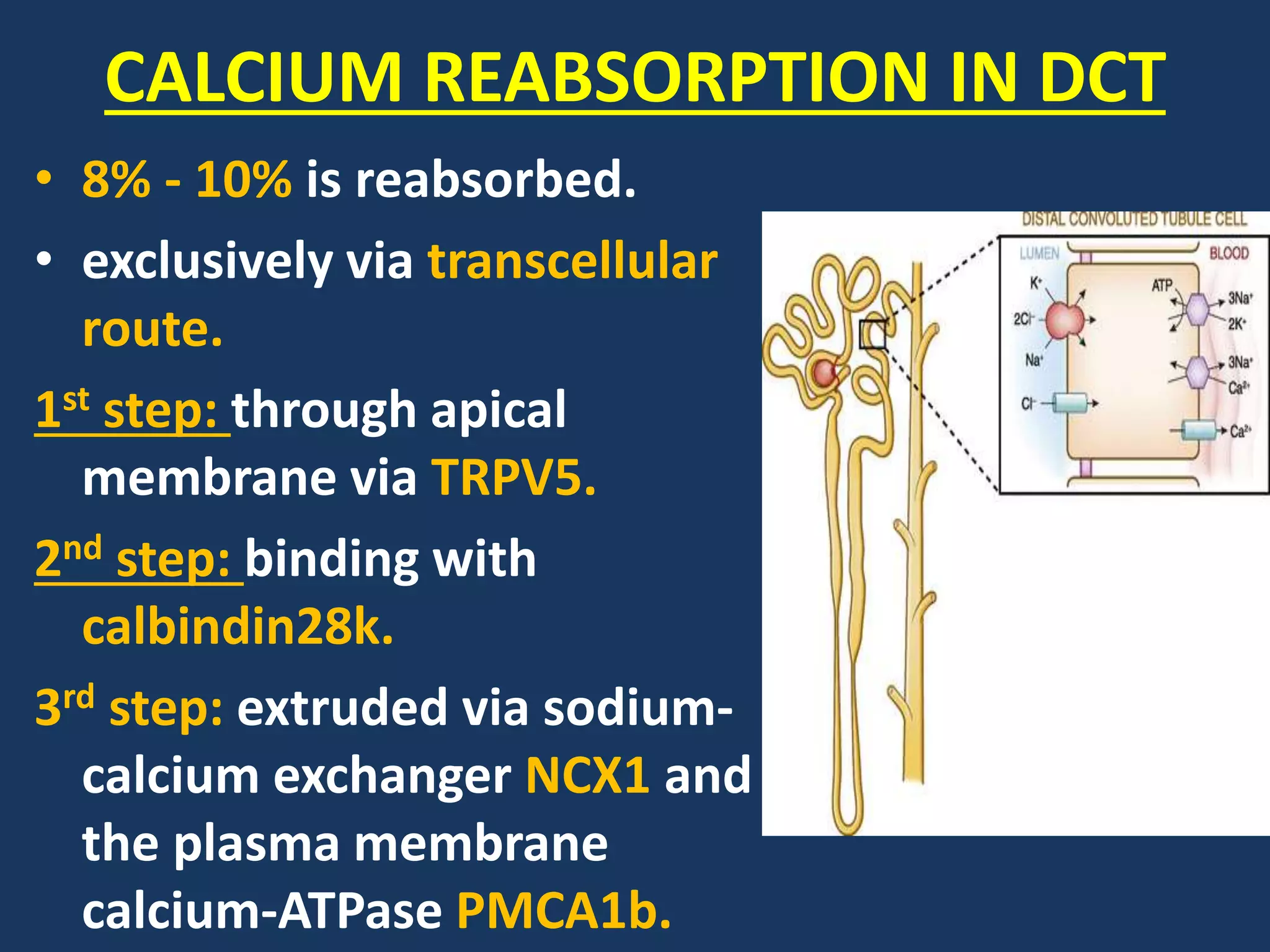
• Calcitriol [1,
25(OH)2D]
stimulates
calcium
absorption.](https://image.slidesharecdn.com/calciummetabolismppt-170820154507/75/Calcium-metabolism-ppt-25-2048.jpg)