Downloaded 1,288 times
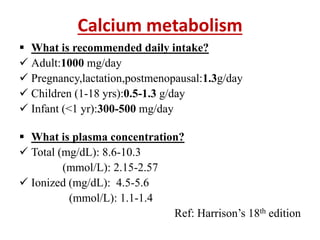
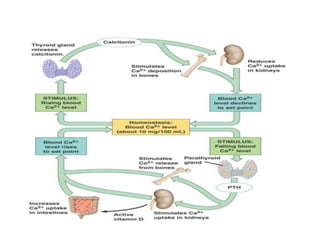
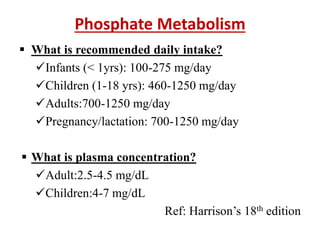

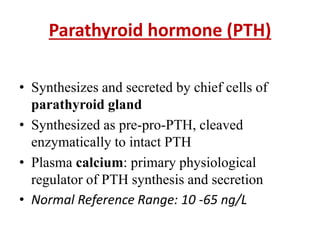
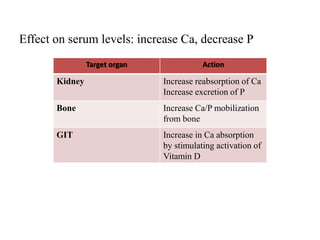


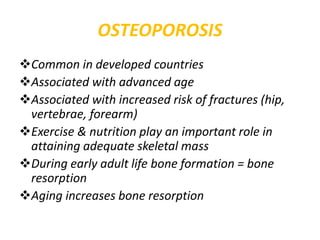
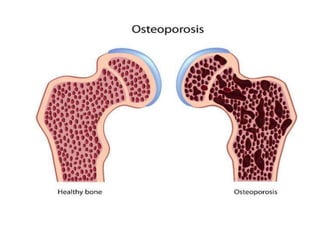
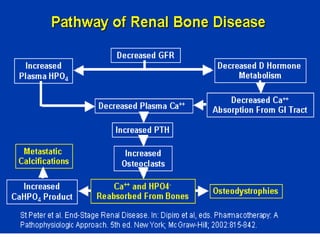


This document discusses metabolic bone diseases, including their composition, calcium and phosphate metabolism, and specific diseases. It provides details on osteoporosis, rickets/osteomalacia, Paget's disease, and renal osteodystrophy. The composition of bone includes collagen, proteoglycans, and hydroxyapatite. Calcium and vitamin D intake recommendations are outlined for different populations. PTH, calcitonin, vitamin D, and alkaline phosphatase roles in calcium regulation are summarized. Osteoporosis risk factors and management strategies are highlighted.












































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)