Downloaded 207 times
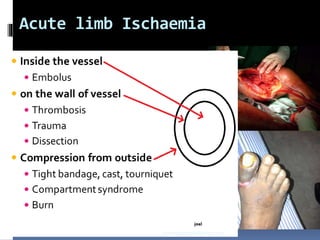
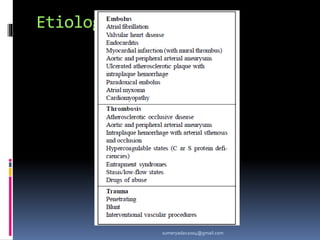

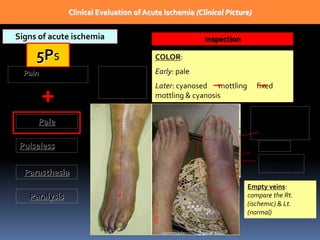
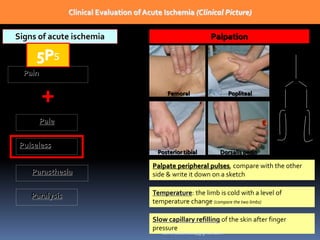
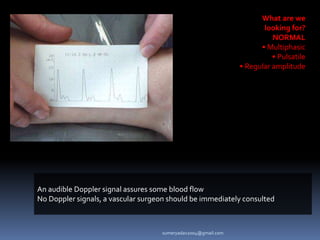
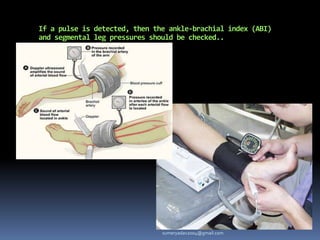
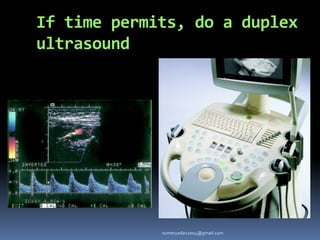
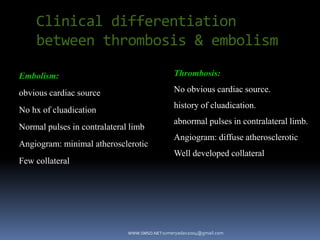
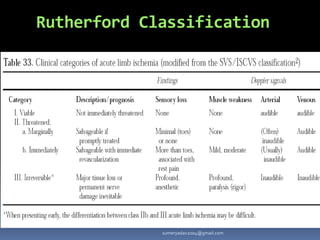
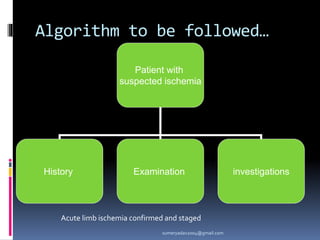
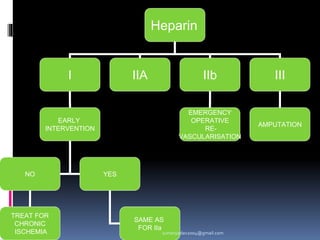
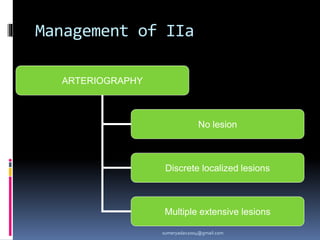
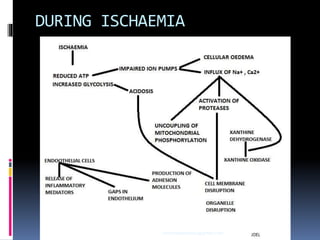
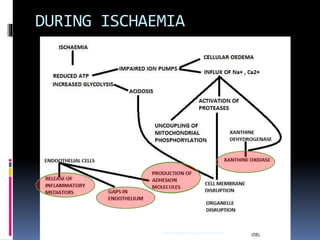
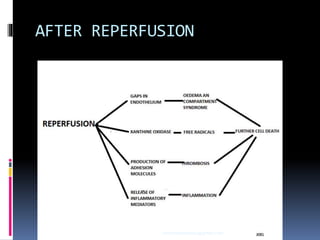
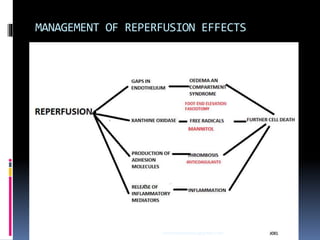
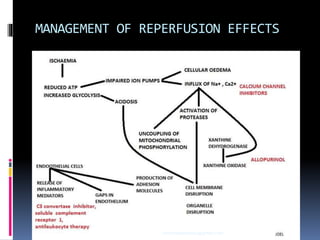
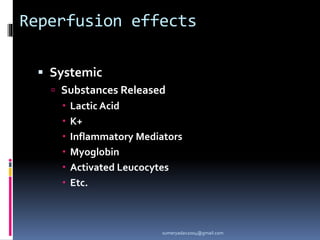



Acute limb ischemia occurs when there is a sudden interruption of blood flow to a limb, threatening the viability of the limb. It can be caused by emboli originating from the heart or blood vessels, or from thrombosis of arteries due to conditions like atherosclerosis. Clinical evaluation focuses on the 5 Ps - pain, pallor, pulselessness, paresthesia, and paralysis. Investigations include Doppler ultrasound, angiography, and measurement of ankle-brachial indices. Treatment involves immediate care, thrombolysis, or surgical revascularization depending on the severity. Complications can include reperfusion injury, compartment syndrome, bleeding, and potential limb amputation.























































































